Slipped capital femoral epiphysis
Table of Contents
What is slipped capital femoral epiphysis?
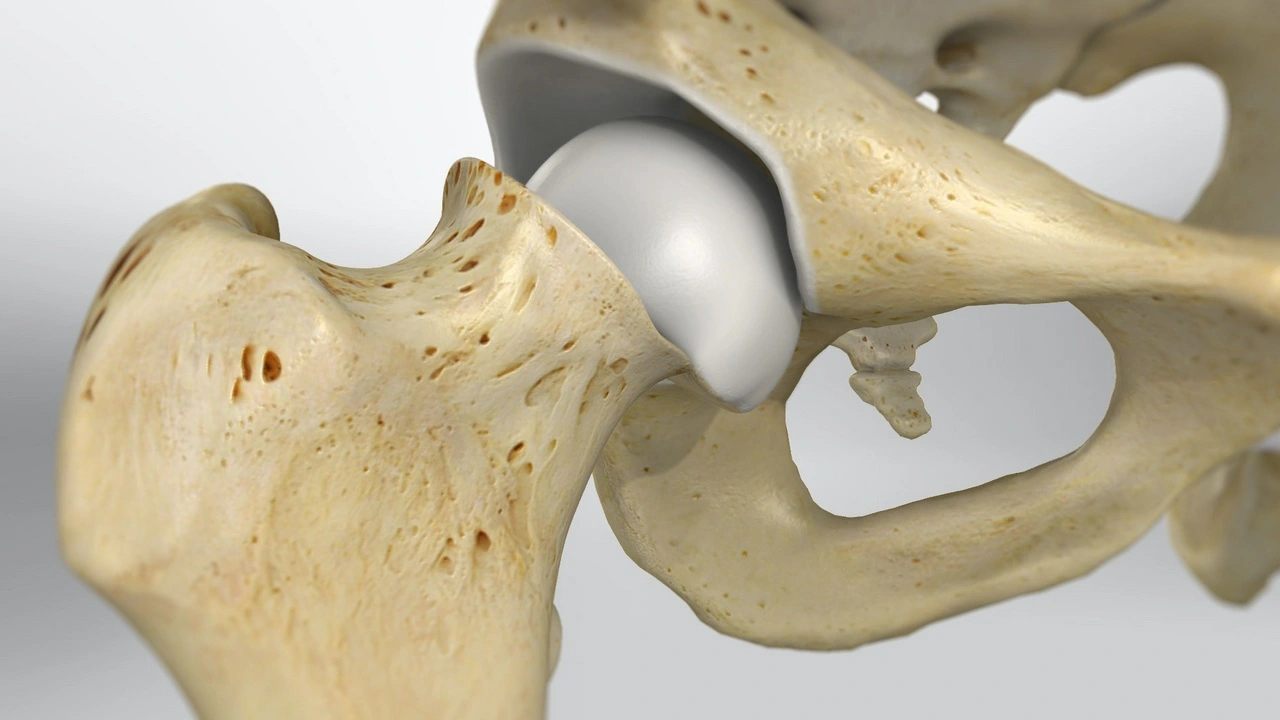
The slipped capital femoral epiphysis is a disorder of adults in which the growth plate of the femoral is damaged and the femoral head slips(moves) with respect to the rest of the femur. The head of the femur stays in the cup of the hip joint, whereas the rest of the femur is shifted.
Different types of the slipped capital femoral epiphysis
There are two types of slipped capital femoral epiphysis, stable and unstable.
- Stable slipped capital femoral epiphysis: With this type, your child can still walk. He will usually have a limp that comes and goes. It’s worse with activity and gets better with rest. Stable slipped capital femoral epiphysis can cause pain or stiffness in the hip, groin, or knee.
- Unstable slipped capital femoral epiphysis: This type is more severe. Your children will not be able to put weight on the affected leg. This type tends to happen suddenly and is severe pain. It can also become a more serious complication.
Causes of Slipped capital femoral epiphysis
The exact cause of SCFE is not unknown. There are many factors that are associated with this condition. These factors lead to the weakening of the growth plate also called the physis which then causes the femoral head ball of the femur to slip off the neck of the femur. Obesity is a major risk factor for this condition. endocrine disorders are risk factors for (SCFE), such as hypothyroidism and osteodystrophy. There might be a genetic predisposition to this condition it runs in families. Boys are more often affected rather than girls.
Signs and symptoms of Slipped capital femoral epiphysis
The patient might have pain in the groin, inner thigh, or knee. They might have stiffness and decreased ability to rotate the leg. Additionally, there might be a change in their gait, or the way they walk, as they try to put as little weight as possible on the affected side. They may also walk with the leg rotated outward.
In most cases, the onset of pain and limp is slow and gradual, whereas symptoms can also occur suddenly and may be associated with a minor fall or trauma.
Differential Diagnosis
Other conditions to rule out:
- Femoral fractures
- Avascular necrosis of the femoral head
- Legg-Calve-Perthes Disease
- Osteomyelitis
- Septic Arthritis
- Groin Strain
- Apophyseal avulsion fracture of the anterosuperior and anteroinferior iliac spine
- Apophysitis of the anterosuperior and anteroinferior iliac spine
- Transient synovitis
Diagnosis
The pediatric orthopedic specialist will obtain a complete medical history and do a thorough physical examination. The patient will also order x-rays which will make the final diagnosis. In rare instances, an MRI might be needed if the x-rays are inconclusive.
- Atypical/Typical
- Loder classification
- Stable
- Unstable is practically defined as when the patient is unable to ambulate even with crutches
- Temporal
- Acute
- Chronic
- Acute-on-chronic
- Radiological
- Grade I = 0–33% slippage
- Grade II = 34–50% slippage
- Grade III = >50% slippage
Complications
- prolong degenerative osteoarthritis: ~90%
- Avascular necrosis of the femoral head (10-15%): increased incidence with the number of attempted reductions and with multiple screws for pinning 3
- Chondrolysis (7-10%): acute cartilage necrosis deformity
- Femoroacetabular impingement: occurs in some patients who have a residual hip deformity post-correction characterized by relative posterior and medial displacement of the capital femoral epiphysis which then leads to an anterolateral prominence of the metaphysis which abuts on the acetabular rim 9
- limb length discrepancy
Slipped capital femoral epiphysis Treatment
The goal of treatment is to prevent the femoral head from slipping any further and to avoid complications. This is accomplished with surgery. A screw is inserted to connect the femoral head with the rest of the femur. If severe deformities are present, the surgeon may decide to realign the bones before placing the screw. The surgeon may also be recommended placing a screw in the unaffected hip to prevent slippage before it occurs.
In some cases, the slip is very unstable (may slip further rapidly) and so it is essential that an orthopedic surgeon sees the patient as soon as possible. In extreme cases, it is essential to perform surgery on the day of diagnosis. However, most slips are stable and can wait 3-14 days for operative treatment.
During the time between diagnosis and surgery, it is important to have the child rest and avoid putting weight on the affected leg. After surgery, the child will only be allowed to put a little weight on the leg and require the assistance of crutches or a walker.
Surgery is needed. The primary goal of surgery is to prevent further slippage and avoid complications. The most common type of surgery is known as ‘screw fixation.’ In this procedure, the surgeon passes a screw from the side of the top of the femur, through the neck of the femur bone, through the growth plate, and into the ‘ball’ section of the femur. The screw keeps the ‘ball’ part of the femur from slipping out of place.
Nonsurgical treatment options can include the RICE approach:
- Resting your leg.
- Apply ice to your knee.
- Compression wraps on your knee to decrease the amount of joint swelling.
- Elevating your leg.
How our physiotherapists can help?
In humans, the hip is our body’s strongest and most stable joint. Any disability in the hip should always be examined as quickly as possible. Senior physiotherapists might be one of the first healthcare professionals to
The therapist will conduct a thorough evaluation that includes this taking a health history having a detailed discussion of the children’s pain symptoms identifying risk factors associated with the conditions of the patient reviewing laboratory tests and imaging studies observing the children’s gait and functional mobility and most vital, conducting a hands-on physical assessment
Treatment for slipped capital femoral epiphysis includes keeping the head of the femur stable and maintaining a lower-extremity range of motion(R.O.M) and strength in order to prevent the development of arthritic conditions in the future. Often, surgery is required to stabilize the bone and promote healing. After the initial diagnosis, children might use crutches til the time of surgery, in order to protect the site until joint alignment is restored.
Evaluation is crucial for guiding the treatment of slipped capital femoral epiphysis.
The therapist will conduct a thorough evaluation that includes this
We work closely with each and every child and their caregivers to develop an individualized treatment program and promote a return to full mobility. We will work with your child to ensure the safe performance of daily living activities, and recommend temporary movement restrictions in the child’s best interest.
Treatment for slipped capital femoral epiphysis includes keeping the head of the femur stable and maintaining a lower-extremity range of motion(R.O.M) and strength in order to prevent the development of arthritic conditions in the future. Often, surgery is required to stabilize the bone and promote healing. After the initial diagnosis, children might use crutches til the time of surgery, in order to protect the site until joint alignment is restored.
After surgery, a follow-up with the orthopedic surgeon is essential to establish recovery and treatment guidelines. Physiotherapy will begin after surgery in order to promote strengthening and return to activity.
- ULTRASOUND THERAPY: Ultrasound is a therapeutic modality that generates ultrasound causes deep heat, provides micro-massage to soft tissue, improves flexibility, promotes healing of tissue as well increases localized blood supply to the area. And ultimately relieving pain.
- SHORT WAVE DIATHERMY(SWD): short wave diathermy is a deep heating modality that gives heat to provide pain relief, it improves the blood supply to the targeted pain area, and removal of waste products.
- TENS: transcutaneous electrical nerve stimulation(TENs) is an electrical modality that provides pain relief by providing pain modulation. It closes the gate mechanism at the anterior grey horn of the spinal cord. Also stimulates the endogenous opioid system which prevents the release of substances at the anterior grey horn.
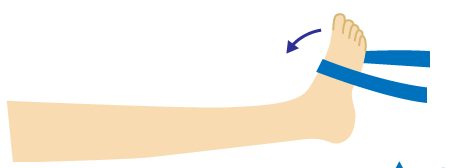
- Sit with your foot dorsiflexed such that the heel is touching the ground. Perform internal rotation of the foot. Can be done with or without a resistance band with a band tied to the forefoot.
- Isometrically perform internal hip rotation with forefoot in sitting on a bar or table.

- Open-chain full ROM of the knee with a resistance band tied on the forefoot laterally resisting internal rotation.

- Close chain proprioception exercise on the Bosu ball with the affected leg fixed on the Bosu ball and perform a cross lunge.

- Single-leg forward jumps with the knee slightly flexed.

Surgical treatment
Surgery is needed for the slipped capital femoral epiphysis. The primary goal of surgery is to prevent further slippage and avoid complications. The most common type of surgery is known as ‘screw fixation’. In this procedure, the surgeon passes a screw from the side of the top of the femur, through the neck of the femur bone, through the growth plate, and into the ‘ball’ section of the femur. The screw keeps the ‘ball’ part of the femur from slipping out of place.
FAQ
How can you fix a slipped capital femoral epiphysis?
SCFE is always treated with surgery to stabilize the growth plate that slipped in the hip joint. But even before the surgery, the doctor will try to prevent any further slipping by encouraging rest and the usage of crutches to avoid putting weight on the affected leg of SCFE.
Is slipped capital femoral epiphysis serious?
Without early detection and proper treatment, SCFE can lead to potentially serious complications, including rapid degeneration of the femoral head and painful arthritis in the hip joint.
What is the common age range for slipped capital femoral epiphysis?
The slipped capital femoral epiphysis is a condition typically affecting adolescents, during the period of rapid growth, from 10-15 years of age.
Does SCFE lead to hip replacement?
In some patients, residual slipped capital femoral epiphysis deformity is associated with advanced osteoarthritis and the only effective treatment may be a total hip replacement.
Does SCFE run in families?
Certain endocrine disorders are risk factors for slipped capital femoral epiphysis, such as hypothyroidism and osteodystrophy. There might be a genetic predisposition to this condition. Boys are more often affected than girls.