Sleeping Rib Syndrome
Slipping rib syndrome (SRS) is a condition of the anterior-lower chest wall characterized by pain in the lower chest or upper abdominal region caused by intercostal nerve impingement as an outcome of abnormal movement of false ribs (8-12) related to unstable coastal cartilaginous attachments.
Table of Contents
Other names for Slipping rib syndrome include:
- Clicking rib
- Displaced ribs
- Rib tip syndrome
- Costal margin syndrome
- Floating rib syndrome
- Nerve nipping
- Painful rib syndrome
- Slipping-rib-cartilage syndrome
- Gliding ribs
- Traumatic intercostal neuritis
- Twelfth rib syndrome
- Cyriax syndrome
- Interchondral subluxation, among others.
Epidemiology
Slipping rib syndrome is a rare condition that affects both males and females of all ages. A review of slipping rib syndrome by Gress et al states that the accessible proof relating to the epidemiology is frequently conflicting and anecdotal.
- It is considered to be a rare syndrome and accounts for roughly 5 percent of all musculoskeletal chest pain in primary care.
- Can takes place at any age, more general in middle-aged female, and is a relatively uncommon, but acknowledged cause of recurrent lower chest and/or upper abdomen pain in adolescents.
- It is been reported in people as young as seven years and as old as 86, but it mostly affects middle-aged individuals.
Clinically Relevant Anatomy
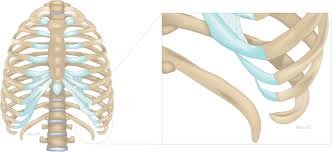
There are 3 types of ribs:
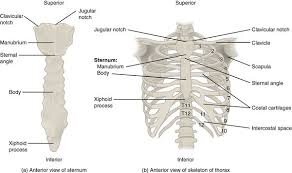
- Ribs which are attached to the sternum by costosternal joints and ligaments (true ribs – 1-7th)
- Ribs that are associated with each other through a weaker cartilaginous or fibrous band (false ribs – 8-10th)
- Ribs that aren’t attached to the sternum or to each other (floating ribs – 11-12th)
- The condition originates from hypermobility of the anterior ends of the false rib costal cartilages, which frequently leads to the slipping of the injured rib under the superior adjacent rib.
- This slippage or motion can lead to an irritation of the intercostal nerve, the strain of the intercostal muscles(Chest muscle strain), a sprain of the lower costal cartilage, or general inflammation in the affected area.
- Because of their delicate connection, there is improved mobility and huge susceptibility to trauma.
- Anterior rib hypermobility is also likely to be the cause of problems in the posterior thoracic area because it is a closed system.
Pathophysiology
- Subluxation of the rib tips caused by interrupted articulation causes the ends of the ribs to nuzzle inside and impinge on the intercostal nerves.
- The impingement causes pain as the outcome of repeated irritation of the intercostal nerves.
Causes of Sleeping Rib Syndrome
It may be caused by:
- Congenital anomaly of the chest wall.
- The destruction of the fibrous articulation of the rib or its cartilage portion.
- Related hypermobility of the costal cartilages of the false ribs.
Risk Factors
Following factors may come up with the risk of developing SRS.
- Overuse
- Direct trauma causes pain.
- Sudden extension or flexion, repeated one-sided weight bearing or exercise like throwing a ball, vigorous swimming, or swinging a bat.
Signs and Symptoms of Sleeping Rib Syndrome
Slipping rib syndrome is come up through the following characteristics.
- Enormous pain in the lower chest or upper abdomen above the costal margin, mostly at the height of the 8th, 9th, and 10th ribs (false ribs).
- A tender spot on the costal margin
- Reproduction of the pain by pressing the pain spot or by external influences
- Signs and symptoms are usually unilateral, however, there are also cases where people reported bilateral pain.
- Below given signs and symptoms may be observed:
- Upper abdominal and lower anterior chest wall pain.
- Flank pain
- Tenderness over the injured coastal margins
- Clicking, popping, or slipping sensations may also be present.
- The pain was increased by some kind of activities like sitting, leaning forward, and interestingly she found that using a swing machine was specifically to generate discomfort.
- Pain connected with slipping rib syndrome has distinct characteristics which may be used in identifying the syndrome:
- Intermittent sharp stabbing pain followed by a constant monotonous pain that can last from a few hours to many weeks.
- The range of severity of pain varies from being a minor nuisance, to moderately severe to interfere with activities of daily living.
- Can also be reported to go from the costochondral area to the chest or to the same level in the back.
- Symptoms are increased by certain postures and movements: lying or turning in bed, rising from a chair, driving, stretching, reaching, lifting, bending, twisting the trunk, coughing, walking, or bearing loads.
- Can affect sporting activities including trunk movements and deep breathing, but in particular running, horseback riding, arm abduction, or swimming. Pain can be severe enough to make patients stop playing sports.
- Visceral innervation converges at the same spinal cord levels as slipping ribs and intercostal nerves and this close connection of the intercostal nerves and the sympathetic system can also cause a variety of somatic and visceral complaints, like biliary or renal colic.
Diagnostic Procedures
Physical Examination
- The physiotherapist looks for a connection between some movements or postures and pain intensity (signs and symptoms), identify if the patient has experienced recent trauma (not usually present), constrained posture, or previous abdominal surgery, and reproduces the symptoms (for example, pain, clicking).
Palpation
- At physical examination, the most usual finding in a case of slipping rib syndrome is tenderness above the costal margin.
- The physiotherapist may reproduce chest pain by palpation.
- A painful click is sometimes felt over the tip of the involved costal cartilage with some movements.
The Hooking manoeuver
- positive test.
- Replicate the symptoms.
- This is a relatively simple clinical test where the physician put his or her fingers under the lower costal margin and pulls the hand in an anterior direction.
- Pain or clicking suggests a positive test
- Intercostal nerve blocks may be performed after positive hooking manoeuver, to confirm the diagnosis.
Dynamic ultrasound of the ribs
- It may be performed with Valsalva, coughing, twisting, crunching, and push maneuvers to diagnose SRS.
Differential Diagnosis
The differential diagnosis of slipping rib syndrome involves a variety of conditions:
- Cholecystitis
- Esophagitis
- Gastric ulcers
- Stress fractures
- Muscle tears
- Pleuritic chest pain
- Bronchitis
- Asthma
- Costochondritis, or Tietze syndrome
- Appendicitis
- Heart conditions
- Bone metastases
- Hepatosplenic issues
- Peptic ulcer
- Renal colic
- Pancreatitis
Treatment of Sleeping Rib Syndrome
In some cases, slipping rib syndrome settle on its own without any kind of treatment if not, the choice of treatment is based on the severity of the patient’s symptoms. There are different manoveour in Conservative and non-conservative management that may be taken into account when treating SRS.
Non-conservative Management
- If the condition preserves or causes severe pain, surgery can be suggested.
- Following surgical procedures may be done.
Partial rib resection
- It can be performed to decrease the symptoms.
Minimally Invasive Repair
- It is done for adult Slipped Rib Syndrome Without Costal Cartilage Excision.
Vertical rib plating with bioabsorbable plates
- Significantly it decreased the rate of recurrence in our early experience.
Conservative Management
Conservative management involves the following:
- Rest.
- Avoiding strenuous activities.
- Applying heat or ice to the involved area.
- Oral medications like NSAIDs.
- Topical analgesics.
- Physical Therapy.
- Nerve blocks.
Oral Medications
- Acetaminophen (Tylenol)
- Nonsteroidal anti-inflammatory drugs (NSAID), such as ibuprofen (Advil, Motrin IB) or naproxen (Aleve)
- Intercostal Nerve Blocks
- If the pain continues despite taking a painkiller below given can be done to reduce the symptoms:
A corticosteroid injection
- To help decrease the swelling.
An intercostal nerve block
- (injection of an anesthetic in the intercostal nerve) to reduce pain. If the pain continues after taking a painkiller following can be done to elevate the symptoms:
Exercises to Avoid
- Because of the inherent instability of joints, exercises that put direct pressure on the chest should be avoided.
- Pushups or exercises that include pitching or throwing motions improve the risk.
- Sports that include the potential for contact with other athletes like football or basketball should be avoided until the condition resolves.
Early Exercise
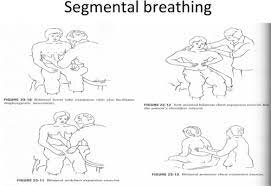
- In the initial stage of recovery, segmental breathing is used to gain more mobility in the ribs.
- Pressure is applied, generally by a therapist, to where the ribs join the sternum.
- The person needs to breathe in and expand the lungs while the pressure is applied.
- The pressure is moved from one segment to another while long tiny breaths are drawn in to put pressure against the therapist’s hand.
Exercise therapy
Expanding Exercises

- To improve the mobility around the rib joints,
- Thoracic extension and flexion
- These exercises may be used.
- In these exercises, arch the back and permit the rib cage to expand, then bend forward and compress the chest and ribs.
- This should only be done to the limits of a person’s comfort.
Seated rotation exercises
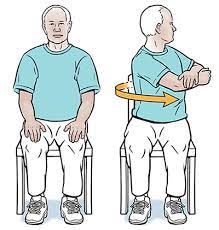
- This can be done by sitting and turning your chest and shoulders as far from one side as you can, like a person is turning and looking over the shoulder, then turning to the other side.
- Use caution and go gently to avoid injury.
Manual therapy
- Manipulation of the costovertebral joint and electric stimulation may help manage the pain, but probably no long-term relief.
Taping

- Tapping of ribs may possibly give some onset relief.
- To decide on the location and direction of taping, give a manual superior compression force through the postero-lateral aspect of the rib cage.
- Now tell the patient to take in a deep breath or rotate.
- If the patient notices a significant improvement in symptoms, then apply the tape at that level.
Rib mobilization with movement (MWM)

- The range of motion and pain level is assessed.
- A cranial glide is given over the lateral aspect of the rib just above the painful region.
- While sustaining this rib elevation (unloading), the patient is asked to rotate again while ROM and pain are once again assessed.
- If there is no significant change, the technique is repeated on a rib above or below.
- If MWM on a rib at a specific level is found to decrease or eliminate the pain, it is repeated ten times.
- A home program of self-MWM can be given.
- Instruction: “lift the rib up with the web space of one hand and actively rotate towards the painful side, repeat as frequently as crucial”.
- The goal is to move the irritated costovertebral joint without pain as often as possible to decrease both the protective muscle spasm and the local inflammation.
FAQ
Symptoms of slipping rib syndrome
Back pain.
Abdominal pain.
Pain in the middle of the chest.
Pain on a person’s side.
Pain in the back of the ribs.
“Popping” or “clicking” experiences, or the sensation that the rib is slipping.
Difficulty breathing because of pain during rib cage expansion and contraction.
Unfortunately, for many, slipped rib syndrome can go undiagnosed for years. The degeneration of nearby cartilage around a rib does not show up on an x-ray, MRI, or CAT scan. The area of the pain is symptomatic for other usual ailments, too.
The discomfort and pain of slipping rib syndrome may make it difficult to live normally. Activities like coughing, bending, lifting, deep breathing, turning in bed, reaching for something, sitting up from a chair, and stretching will often worsen the symptoms.
It is important to remember that person should not start an exercise routine for broken ribs recovery until the doctor says it is safe to proceed. For the primary post-injury recovery, focus on rest. The person needs to rest to best manage the pain and inflammation and let the ribs begin to mend.
The stress and muscle tension caused by anxious behavior could play a role, as chest tension and stress may be a factor. However, anxiety (or other mental illnesses) is not identified as a cause at this time.