
Scapula Fracture (Shoulder Blade Fracture)
Table of Contents
Introduction
The scapula also known as the shoulder blade is a big triangular bone that presents postero-lateral on the upper back or thoracic cage and attaches with the clavicle. The scapula, concurrently with the clavicle and humerus from the shoulder joint, is well linked by a complex system of muscles. Shoulder blades join the arm to the thorax while the muscles of the scapula provide correct arm movement over the thorax.
Scapula Fracture or Shoulder Blade Fracture: Scapular fracture is a not very common fracture that is frequently caused by direct trauma from the back or side.
A scapular fracture means less than 1 percent in the majority among all other fracture bones and 3 percent to 5 percent of all shoulder girdle fractures. eighty percent to ninety-five percent of all fractures of the scapula are treated by other damages for example fractures of the shoulder, collarbone, and ribs, or during damage to the skull, lungs, and spinal cord, generally due to it requiring high-energy or torque trauma to cause an injury to the scapula.
Scapular fractures happen during high-impact trauma for example road traffic accidents, falls, and other high-impact traumas. Road traffic accidents comprise more than 70 percent of scapular fractures, with more than fifty percent correlated with drivers and eighteen percent correlated with walkers struck by motor vehicles.
Other documented modes of cause contain electric shock and seizure due to forces on the scapula. Isolated scapular fractures are exceptionally unique.
Classification of scapular fractures
One or more parts of the scapula can get fractured:
- Scapular body (forty-five percent of patients): transverse, oblique, and longitudinal are the three kinds of the body of the scapula fractures
- Scapular neck (twenty-five percent of patients): Three kinds of neck fractures are described as follows: fracture of the surgical neck, fracture of the anatomical neck, and fracture of the neck below the scapula spine
- Glenoid (35 percent of patients)
- Acromion Process (8 percent of patients)
- Coracoid Process (7 percent of patients)
Causes of a scapular fracture
Scapular fractures or fractures of shoulder blades are commonly due to direct trauma involving an extreme amount of force, accordingly in greater than seventy-five percent of scapular fracture cases, there are other corresponding injuries to the chest, lungs, and internal organs.
- Motor vehicle accidents
- Falls with direct trauma to the shoulder
- Falls onto an outstretched arm
- Blunt trauma like from a baseball bat or hammer
- Fall from height
- Contact sports
- Direct blow to the scapula
Symptoms of the fractured scapula
- Localized pain at rest
- Extreme pain when moving the arm
- Tenderness
- Swelling around the back of the shoulder
- Extreme bruising and scrapes close to the damaged place
Extreme bruising and scrapes nearby the affected region - Holding the injured arm close to the body where the shoulder is in a 90-90 degree position with elbow with shoulder internal rotation.
- Inability to lift the arm
- Flattened and deformed shoulder appearance
- Pain during breathing because of related chest wall trauma
- The abnormal sensation of numbness, tingling, or coldness of the arm because of impaired blood circulation and nerve supply
- Crepitus and popping sensation at the end feel of the shoulder joint motions
Evaluation of scapular fractures
Diagnosis of a fractured scapula is likely only after a good physical assessment and examination.
- The first step is to examine and evaluate the position and posture of the shoulder joint.
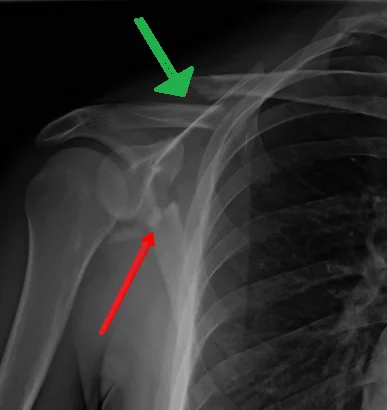
- In the scapula, multiple fracture cases are distinctly seen in a shoulder and chest X-ray but can readily be overlooked during the X-ray inspection.
- 80% of the time scapular fracture is associated with other severe injuries which need to be taken into account during patient assessment. Few of this trauma can be potentially life-threatening. As thoracic-scapular dissociations with disruptions of the subclavian vein and axillary vessels can show to life-threatening hemorrhage.
- CT or MRI investigation can be a must particularly to diagnose the fracture of the glenoid which incorporates thirty-five percent of all scapular fractures.
- MRI will reveal a clean visual of the severity of injury to the nearby soft tissue, joints, ligaments, and nerves.
Differential diagnosis of scapular fractures
Christopher Libby; Nicholas Frane; Thomas P. Bentley. have expressed the subsequent potential cases of differential diagnosis in their investigation”Scapula Fracture”.
- Abdominal Pain in elderly people
- Acromioclavicular injury
- Fractures of clavicle
- Mechanical back pain
- Pneumothorax
- Rib Fracture
- Shoulder Dislocation
Management of scapular fractures
Around more than eighty percent of scapular fractures are un-displaced fractures, therefore scapular fractures are excellently operated without operation procedure, and fractures with minor or no displacement recover in the absence of any major difficulties.
Fractures of the body of the scapular with displacement can recover with malformation, but the scapular parts are musculature in a manner that actually can not interrupt the activity of the involved shoulder. Regardless, displaced fractures in the scapular processes or in the glenoid area, do interrupt movement in the engaged shoulder if they are not repositioned appropriately.
Accordingly, while several fractures of the scapular are treated without operation, reduction by surgically is demanded for fractures in the neck or the glenoid; otherwise, the ROM of the shoulder joint may become deformed.
Medical Treatment
Pain after an injury or operation is a natural portion of the curative process. Medications are oftentimes recommended for short-term pain to ease afterward injury or operation.
Different types of drugs are present to aid in the minimization of pain, for example, opioids, non-steroidal anti-inflammatory drugs (NSAIDs), and regional analgesics. Physicians may prescribe a type of these drugs to improve pain relief, as well as minimize the need for opioids.
The medical group as well as the patient requires to be conscious that although opioids assist ease pain after an damage or operation, they are a narcotic and can be addictive. Opioid dependence and excessive quantity have become critical public health problems in the United States and around the globe. It is significant to use opioids only as prescribed by the doctor or surgeon. As shortly as a patient’s pain begins to enhance, one should stop taking opioids.
Non-surgical or conservative Treatment
Nonsurgical treatment with a shoulder immobilization splint functions most pleasing for several fractures of the scapula. The splint keeps the shoulder in place while the bone recovers. Immobilization using the sling is normally held in place for six to twelve weeks as that’s how long it takes for the fracture to recover. Ice application is meant to minimize swelling.
Surgical Treatment
The scapula has a select muscular envelope which allows significant recovery of scapular fractures in more than eighty-five of the circumstances. The scapula has a select muscular envelope which allows significant recovery of scapular fractures in more than eighty-five of the circumstances. In multiple cases, scapular malformation can significantly impair the shoulder girdle function, resulting in excessive pain, deformities, impingement syndrome, and scapulothoracic dyskinesis.
Specific kinds of scapular fractures that can require operation are:
- Displaced fractures of the glenoid articular surface
- Fracture of the scapula neck with angulation
- Fractures of the acromion process that cause the arm bone to hit in front of it (impingement syndrome)
Postoperative Care:
- A bandage is present where the shoulder is operated, and the operated arm is set in a splint to keep the shoulder in support.
- The application of ice to relieve pain and minimized swelling is recommended.
- The incision is to be maintained neat and dry at all times.
- Precise instructions about movement and rehabilitation are to be delivered to the patient.
- Physiotherapists are instructed to correct shoulder function and strength and it is critical that the patient obeys the exercise plan put in place by the physiotherapist to enhance motion and strength in the shoulder and avoid stiffness.
- The patient is asked to eat a healthy diet and not smoke or drink at least during the stage of recovery along with taking medications as prescribed.
Risks and Complications of Surgery:
Bleeding, infection, anesthetic reactions such as fever or nausea, blood clots or deep venous thrombosis, damage to nerves and blood vessels, shoulder stiffness, fat embolism, failure to heal properly, and the need for repeat surgery.
Rehabilitation
Earlier physiotherapy with exercises developed to enhance the range of motion of the shoulder joint is necessary. It is necessary to begin these exercises early to prevent adhesive capsulitis. Lack of movement in the shoulder can happen if the shoulder joint is not operated for a long duration. It is advisable to begin moving your shoulder within the first week after the injury to decrease the chance of shoulder and stiffness of the elbow. Exercises must be continued until full shoulder movement returns. This can also take 6 months to 1 year.
Initial exercises are begun within the first- and second-week post-injury as guided by the physiotherapist provided there is no increase in pain due to the exercises.
Exercises for the uninvolved joints can be begun within the first two days of injury.
Week zero to three – Stage 1 Exercises
- Hand open and close
- Wrist flexion to extension
- Elbow flexion and extension in the pain-free range
- Forearm rotation
Week three to six – Stage 2 Exercises
- Shoulder pendular exercises
- Active assisted shoulder flexion
- Actively assisted shoulder abduction
- Active assisted external rotation
After week six – Stage 3 Exercises
- Active forward flexion of the shoulder
- Active shoulder abduction
- Active external rotation of the shoulder
- Strengthening exercises for the upper limb by utilizing load and resistance bands.
- Shoulder retraction exercise – also named shoulder blade squeeze
- Wall push-ups
- strengthening of the rotator cuff: Static rotator cuff – push in and push out
External rotation of the shoulder using a resistance band
Note: All exercises are to be repeated ten times each, four-five times a day. The patient is recommended only to go as far as he or she can inherently go without doing any trick movements to try and get further. The ROM will improve over time and must not be pushed.
FAQ
This fracture kind is commonly treated with non-surgical methods. Yet, they may need an operation in a few conditions depending on its severity. Shoulder blade fractures can typically cause due to extreme injuries to the chest, lungs, and internal organs.
Various fractures of the scapula can be managed without operation. Treatment includes rest and immobilization with a sling or a shoulder immobilizer, cryotherapy, and pain drugs. The sling is normally maintained for convenience for the first two weeks with a following increase in the shoulder’s ROM.
In kind-III fractures, the impact is directed relatively superiorly, with the fracture line running along the superior border of the scapula and occasionally disrupting a few structures of the superior shoulder suspensory complex(SSSC). The fractured segment contains the coracoid process and the superior articular surface of the glenoid cavity
Holding the fractured bone beyond your heart avoid blood from pooling and resulting in swelling. First, try sleeping on your back while keeping yourself on various pillows. If this doesn’t help, modify gradually to the side lime position if comfortable. Sleep in the center of the bed, so you don’t slip in the middle during sleep.
Home Care
Place ice on the shoulder region for 15 minutes, then leave it off for fifteen minutes. Do this three to four times a day for two to three days. …
Rest your shoulder for the next following days.
Gradually return to your regular activities. …
Taking ibuprofen or acetaminophen (for example Tylenol) may assist control inflammation and pain.
The levator scapulae, or shoulder-shrugger muscles, can occasionally sense locked up, provoking pain in the neck and shoulders. To perform them, cover an arm around yourself to touch the top inside corner of your contrasting shoulder blade. Press on the knots and move back and onward with the help of your digits.




One Comment