
Scalene Muscle
Table of Contents
What is Scalene Muscle?
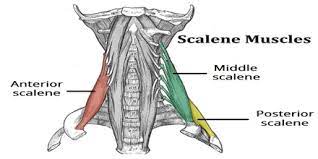
- The scalene muscle are the 3 muscles situated on each side of the neck, spanning between the transverse processes of the cervical vertebrae & the upper 2 ribs. Namely, these muscles are the scalenus anterior (anterior scalene), scalenus medius (middle scalene), & scalenus posterior (posterior scalene). They are all relates to the lateral vertebral muscle group.
- The primary functions of these muscles are flexion, lateral flexion, & rotation of the neck. Moreover, they are the suppository muscles of respiration, elevating the ribs during forced inhalation.
Anterior Scalene Muscle
What is Anterior Scalene Muscle?
- The anterior scalene, AKA scalenus anterior (scalenus anticus; in Latin: musculus scalenus anterior) muscle is 1 of the lateral muscles of the neck, relating to the scalene group. It is deeper situated, lying beside the Sternocleidomastoid SCM.
- It is situated between the subclavian vein & the subclavian artery. The roots of the brachial plexus cross posterior to it. The phrenic nerve passes its anterior surface.
Relations of Anterior Scalene Muscle
- The scalenus anterior muscle is situated in the lateral part of the neck, anterior to the subclavian artery, & posterior to the phrenic nerve. It is liable to more structures of the neck;
- Posteriorly, it is reliable to the suprapleural membrane, pleura, roots of the brachial plexus, & the subclavian artery.
- Anteriorly to the muscle are the:
- Clavicle, subclavius, sternocleidomastoid, & the omohyoid muscle
- The lateral portion of the carotid sheath, transverse cervical, suprascapular & ascending cervical arteries, subclavian vein, prevertebral fascia
- C3 – C5 spinal roots form the phrenic nerve right on the anterior aspect of the scalenus anterior.
- The scalenus anterior muscle is made up of the anterior border of the inter scalene (scalene) triangle. The posterior border of this space is made up of the scalenus medius, while the inferior border is made up of 1st rib. This space is very necessary as it is traversed by the trunks of the brachial plexus & the 3rd segment of the subclavian artery.
Origin
- The scalenus anterior muscle is the inner-most/anterior-most of the 3 scalene muscles. It begins from the anterior tubercles of transverse processes of the vertebrae C3 to C6. The muscle takes an inferior, almost vertical, diverge towards the thoracic cage. It gives off a single flat tendon, that ends into the scalene tubercle & superior border of the 1st rib, just anterior to the groove for the subclavian artery.
Insertion
- The scalenus anterior muscle occasionally gives off a few muscular slips that end in the suprapleural membrane. These slips are termed the scalenus minimus (pleuritis) muscle, the Albinus muscle, or Sibson’s muscle. It is a normal anatomical variant present within 7 to 46% of people.
- When present, the scalenus minimus muscle begins from the anterior border of the transverse process of the C7 vertebra. It ends into the inner border of the 1st rib behind the groove for the subclavian artery, with a less number of slips also joining to the pleural dome. Due to its pleural joining, it is predicted that this muscle tenses the pleural dome.
Nerve Supply
- The scalenus anterior muscle collects its innervation from the anterior rami of the spinal nerves C4 to C6.
Blood Supply
- The vascular supply to all scalene muscles arrives from the ascending cervical branch of the inferior thyroid artery. The inferior thyroid artery own is an indirect branch of the subclavian artery through the thyrocervical trunk.
Action
- It works as a Bilateral contraction – neck flexion
- It works as Unilateral contraction – neck rotation (contralateral), elevates rib first, neck lateral flexion (ipsilateral)
The function of the Scalene Anterior Muscle
- The scalenus anterior muscle movement on the joints between the cervical vertebrae. Depending on the location of the head & the type of muscle contraction, the scalenus anterior can generate the following movements:
- When the costal joining is fixed, bilateral contraction of the muscles produces the flexion of the neck.
- When the head is in the anatomical posture (upright & facing anteriorly), unilateral contraction of the muscle produces ipsilateral flexion of the neck (to the same side).
- When their joining to the vertebral column is stable, the scalenus anterior muscles have the ability to fix or lift the 1st rib superiorly.
- Together with the contraction of the external intercostal muscles which elevate the ribs two to twelve, this action of the scalenus anterior enlarges the anteroposterior diameter of the thorax. However, the muscle works this way only during forced breathing, which makes it an assist respiratory muscle, either than a primary respiratory muscle.
Scalenus medius muscle
What is Medius Scalene Muscle?
- Middle Scalene, AKA Scalenus Medius (in Latin: musculus scalenus medius), is the biggest/largest & longest muscle in the scalene group of lateral neck muscles. Often penetrated by the dorsal scapular & long thoracic nerves, it is deeper situated, lying beside the Sternocleidomastoid.
Relations of medius Scalene Muscle
- The anterolateral aspect of the scalenus medius is surfaced by the sternocleidomastoid muscle. The lower half of the muscle is passed by the omohyoid muscle, clavicle, subclavian artery, & anterior rami of the cervical spinal nerves. The anterior surface of the muscle is penetrated by the dorsal scapular nerve & the nerve to the serratus anterior muscle.
- These nerves start on the lateral surface of the muscle &continue towards the rhomboid’s seven serratus anterior, which they supplied, respectively. The posterolateral surface of the muscle is reliable to the levator scapulae & the scalenus posterior muscle.
Origin
- The scalenus medius muscle is the biggest & the longest of the scalenes. It begins from the transverse processes of the axis (C2), transverse processes of the atlas (C1), & the posterior tubercles of transverse processes of the vertebrae C3 to C7.
Insertion
- The muscle fibers straighten posterolaterally to create a tendon, which ends in the superior border of the 1st rib. The end site is situated posterior to the groove for the subclavian artery & anterior to the tubercle of the 1st rib.
Nerve Supply
- The nerve supply to the scalenus medius muscle is supplied by the anterior rami of cervical spinal nerves C3 to C8.
Blood Supply
- Like the scalenus anterior, the scalenus medius collects its blood supply from the ascending cervical branch of the inferior thyroid artery.
Action
- It works as Neck lateral flexion raises the rib first
The function of Scalene Medius Muscle
- The squeezing of the scalenus medius muscle produces a strong ipsilateral flexion of the neck. In the same manner, as the scalenus anterior, this muscle assists to stabilize or elevate the first during breathing, when its vertebral joining is fixed.
Scalene Posterior Muscle
What is Posterior Scalene Muscle?
- Posterior Scalene, AKA Scalenus Posterior, is 1 of the lateral muscles of the neck, relating to the Scalene group. It is deeper siuated, lying beside the Sternocleidomastoid muscle.
Relations of Scalene Posterior Muscle
- The posterolateral surface of the muscle is reliable to the levator scapulae & the scalenus posterior muscle.
Origin
- The scalenus posterior is the tiniest of the scalene muscles. Its fibers begin from the posterior tubercles of transverse processes of cervical vertebrae C5 to C7.
Insertion
- The muscle enlarges to the posterolaterally & tapers into a thin tendon, which inserts into the external surface of the 2nd rib. The site of the ending point is situated posterior to the joining of the serratus anterior muscle. Occasionally the fibers of the scalenus posterior can be mixed with the fibers of the scalenus medius.
Nerve Supply
- The scalenus posterior muscle is a nerve supplied by the anterior rami of spinal nerves C6 to C8.
Blood Supply
- Like the other scalenes, the scalenus posterior collects its blood supply from the ascending cervical branch of the inferior thyroid artery. In addition, it collects some vascular supply from the superficial branch of the transverse cervical artery, a branch of the thyrocervical trunk.
Action
- It works as Neck lateral flexion,
- It also Elevates rib two
The function of Scalene Posterior Muscle
- When the costal joining of the scalenus posterior muscle is stable, the unilateral work of the muscle results in the ipsilateral lateral flexion of the neck.
- When the vertebral joining is stable, the muscle helps to steady or elevate the two rib breathing.
Clinical Significance of Scalene Muscle
Torticollis:
- This condition is also termed a wry neck.
- In this condition, it causes the neck muscles, consisting of the scalene muscles, to be constantly contracted in a short position.
- It results in a tilted head from unilateral scalene spasms and rigidity.
Forward head posture position:
- This condition is also termed text neck
- This condition generally occurs in sitting at a computer, driving, dentistry & any position where the head is forward while the shoulder joint is hunched over for extended periods.
- Consequence becomes noticeable with the strained muscles of the neck & worsened posture.
Breathing:
- These scalene muscles are accessory muscles for breathing.
- During inhalation, the scalene muscles lift the upper ribs which is create a volume in the chest cavity.
- When The scalene muscles are contracted, it is open to space for the lungs which is to expand the thorax by lifting the top ribs.
- If occur to any respiratory issues the scalene muscles begin to work harder, which produces tension & tightness.
Scalene syndrome:
- In the Scalene syndromes are compressions of structures around the neck area.
- This syndrome involves the anterior & middle scalene muscles, which become too tight & squeeze the neurovascular components which are located between the two muscles.
- This condition is common with some activities where the head is forward & downward like computer & dental work.
- When your head forward & rounded shoulder posture is greatly affected by the causing of chronic shortening of the scalene muscles.
- This condition can also contribute to thoracic outlet syndrome.
Scalene myofascial pain syndrome:
- This common type of myofascial pain syndrome is a painful condition that originates in the neck & radiates down the arm.
- This syndrome is primary/secondary.
- The Primary pain syndrome condition gives to results from the chronic overuse of the scalene muscles, poor posture & repetition in the microtrauma.
- In Secondary pain, syndrome conditions give to result from medical issues such as osteoarthritis, trauma & complex regional pain syndrome.
- This condition is produce muscle weakness & stiffness which is limit the movement of the neck
Thoracic outlet syndrome:
- There are available to multiple causes of thoracic outlet syndrome, but which is associated with the scalene muscles is when the brachial plexus & subclavian artery are compressed between the anterior & medial scalene muscles.
- This syndrome is produced by weakness, pain, tingling & numbness of the shoulders, upper arm, elbow, forearm, hand & fingertips meaning the whole affected upper limb.
Cervical radiculopathy:
- This condition is also more commonly known as the pinched nerve.
- When the scalene muscles have become too tight, which is produced to narrow the brachial plexus pathway & trap a nerve, which is causing a pinched nerve in the neck so that it is felt through the arm at to the hand.
- When this Scalene muscles become tight, which pinch the structures of the nerves, arteries & veins which is pass through the area to cause burning, tingling, aching & numbness in the arm & neck.
Massage for the Scalene Muscles pain
- For pain relief massage is also applied to the area of pain & points which is the muscle tenderness & trigger points of muscle pain.
- The stroke of massage occurs in an upward to the downward direction or else vice versa can be done.
- This massage helps to relieve tension & pain.
- This massage is applied with to help of oil & powder.
- The message type for this muscle pain is also applied to MFR on the trigger points of release of the muscle pain.
Stretching for the Scalene Muscles pain
Stretching helps you release muscle pain, tightness, or spasms of muscle.
Position for stretching :
- Lower & anchor the shoulder joint of the side to be stretched by placing the side’s hand under the buttock.
- Then Bring the opposite hand over the head so that the fingers make contact with the top of the ear.
- Gently pull the head & neck so that it is tilted to the opposite side of the side which the side wants to stretch then relax the neck muscles.
- Then Try to pull the ear down to the shoulder joint
- Now, the patient is rotating the head & the degree of rotation is used to determine the target scalene muscle.
- Stretch for Posterior Scalene muscle
- To target the posterior scalene muscle, turn the face toward the arm which arm is the pull.
- Stretch for Anterior Scalene muscle
- To target the anterior scalene muscle, turn the face away from the pulling arm.
- stretch for Medial scalene muscle
- To target the middle scalene muscle, look straight up at the ceiling & just slightly toward the pulling arm.
- Then Concentrate on the muscle with the help of your efforts on the muscle & stretch the muscle till you feel the stretching filling.
- Then Hold this stretching position for around 30 seconds & do the 3 times in 1 session & perform 3 sessions per day.
Strengthening exercise for the scalene muscle
- Scalene PNF strengthening
- Strengthen the scalene exercise
Scalene muscle PNF strengthening:
- For strength, the scalene muscle sits in a comfortable chair.
- Then Place the palm of the right hand on the right side of the head.
- This hand acts as a stabilizer for this exercise.
- Then start to move the right ear toward the right shoulder joint while maintaining the resistance which is provided by the right hand.
- Repeat this exercise 8 to 12 times on every side.
- By strengthening this scalene muscle, the patient increases the ability to stabilize the cervical spine, which reduces the risk of a future injury.
Strengthen the scalene exercise:
- The patient is sitting & stands up straight with the resistance band looped around the head.
- Then Hold the ends of the band firmly to one side ensuring there is some tension in the band.
- Pull the band away from the head, resisting the movement by keeping the head in a neutral position.
- Hold this exercise position then relax & repeat this exercise.
Breathing Exercises
Diaphragmatic Breathing Exercise
In supine position
- Lying on your back on a surface or in bed, together with your knees flex and your head supported to the bottom. you’ll use a pillow behind your knees to support the legs.
- Place one hand on his higher chest and therefore the alternative slightly below your skeletal structure. as you’re feeling your diaphragm move as you breathe.
- Breathe in slowly exploiting your nose so your abdomen moves away and it’ll permit your hand to rise. The hand on your chest ought to persist as still as connected
- Tight the abdominal muscles and allow them to fall within as you expire exploitation of your lips. The hand on your belly ought to move down to its original position
- In a sitting position in a chair, with your knees flex and your shoulders, head, and neck neutral position. you can perform for 7 to 10 minutes, several 5 to 6 times a day. Diaphragmatic exercise also call a relation exercise
In sitting position
- Sitting in a chair straight position and lengthen the distance between your umbilicus and sternum.
- your shoulders and neck should be relaxing.
- the pelvis is in the neutral position.
- your hand’s position should be at the side of your lower ribs.
- Breathe in slow using your nose. As you inspirited feel your ribs should be outwards and upwards. During inspiration expansion of the trunk in three areas forward, sides, and back. expiration using your nose. As you expire your lower ribs move inward direction.
Segmental Breathing Exercise
Lateral costal expansion
- it is also called lateral basal expansion. it was usually done unilaterally or bilaterally. it can also be done in a sitting or lying position
- place your hand lateral aspect of the rib cage
- and ask the patient to breathe out and the rib cage should be downward and inward
- as the patient expired therapist should apply pressure on the rib cage with the palms of your hand
- before inspiration, you need to downward and inward stretch to the chest to facilitate the external intercostal contraction
- apply normal force on the lower rib cage to get stimulate and patient to get inspirited deeply and the chest will expand
- when the patient expiration therapist will squeeze the rib cage downward and the inward
- the patient may perform manually and ask to apply force with his hand or with a towel.
Posterior basal expansion
- This form of deep breathing exercise accent post-surgical maneuvers who have bedridden and cannot sit up for a prolonged time period. because of that time secretion move to the posterior segment of the lower side of the rib.
- sit and lean onward on a pillow, slightly bend your hips
- place the physiotherapist’s hand over a posterior segment of the rib
- place your hand lateral aspect of the rib cage
- ask the patient to breathe out and the rib cage should be downward and inward
- as the patient expired therapist should apply pressure on the rib cage with the palms of their hand
- before inspiration, you need to downward and inward stretch to the chest to facilitate the external intercostal contraction
- apply normal force on the lower rib cage to get stimulate and patient to get inspirited deeply and the chest will expand
- when the patient expired therapist will be squeezing the rib cage downward and an inward
- the patient may perform indirectly ask to apply force with his hand or with a towel
Right middle lobe expansion(lingual expansion)
- the patient is in a sitting position therapist’s hand should be right or left side at the below axilla level
- ask the patient to breathe out and the rib cage should be downward and inward
- as the patient expired therapist should apply pressure on the rib cage with the palms of their hand
- before inspiration, you need to downward and inward stretch to the chest to facilitate the external intercostal contraction
- apply normal force on the lower rib cage to get stimulate and patient to get inspirited deeply and the chest will expand
- when the patient expiration therapist will squeeze the rib cage downward and the inward
- the patient may perform manually and ask to apply force with his hand or with a towel
Apical expansion
- Patient in a sitting position on a chair or bed therapist’s hand should be below the clavicle
- As the patient breathes out apply pressure with the palm or fingertip just below the clavicle
- Sitting with using your back straight or lying down. Relax each shoulder and neck the maximum amount as potential.
- inspiration using your nose for two to three seconds, the air is getting into your abdomen. fill your abdomen with air instead of your lungs.
- Purse your lips like you’re processing hot food then expire slowly, taking double as long to exhale as you took to respire.
- you can repeat For several times. you’ll rise the inspiration and expiration counts from a pair of seconds to four seconds, and so on pursed lip breath effective.

5 Comments