
Rigidity
Table of Contents
What is Rigidity?
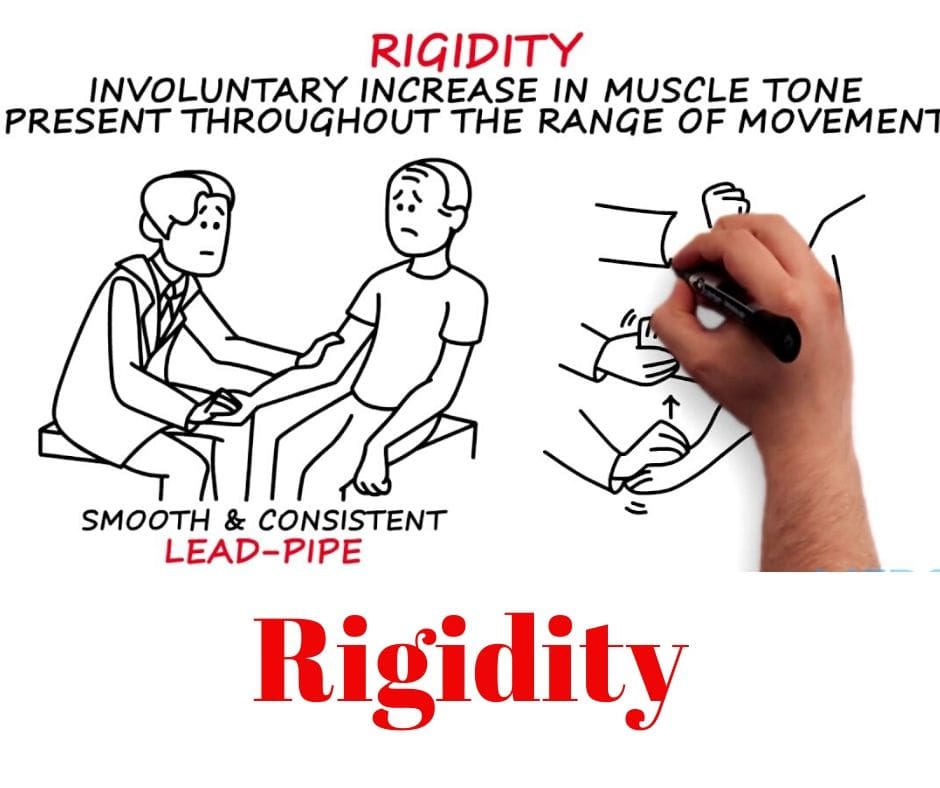
- Rigidity, frequently used as a synonym for Hypertonia by many authors, is a common muscle tone disease in which there is resistance to passive movement irrespective of posture and velocity.
- It is one of the cardinal features of Parkinson’s Disorder and is usually present in extrapyramidal diseases. It affects the agonist muscles and the antagonist’s muscles equally.
It can be seen in –
- Parkinson’s Disease
- Corticobasal Degeneration
- Huntington’s Disease
- Multiple System Atrophy
- Stiff Man/limb Syndrome
- Niemann-Pick Disease – Type A
- Orthostatic Hypotonia Shy-Drager Disease
- Spinocerebellar Ataxia – type 43, 17, 2
Definition
- Rigidity is a hypertonic state characterized by continual resistance throughout ROM that is independent of the velocity of movement. It is the effect of excessive supraspinal drive acting on alpha motor neurons; spinal reflex mechanisms are generally normal. In parkinsonian rigidity, tendon jerks are generally normal.
‘Rigidity’ is determined as hypertonia in which all of the following are true:
- The resistance to externally imposed joint movement is present at very low(mild) speeds of movement, does not depend on imposed speed, and does not exhibit a speed or angle threshold
- Simultaneous co-contraction of agonists and antagonists may occur, which is reflected in an immediate resistance to a reversal of the direction of movement about a joint area.
- The limb does not tend to back to a particular fixed posture or extreme joint angle.
- Voluntary activity in distant muscle groups does not lead to involuntary movements about the rigid joint area, although rigidity may worsen.
Related Anatomy
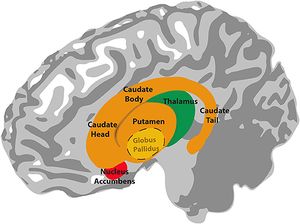
- The “basal ganglia” refers to a group of subcortical nuclei responsible primarily for a motor control function, as well as other roles(functions) such as motor learning, executive functions and behaviors, and emotions. The classical basal ganglia model shows how information flows through the basal ganglia and returns to the cortex through two pathways with opposing results for proper movement execution.
Pathology
- Rigidity is the result of excessive upper motor neuron facilitation acting on alpha motor neurons; spinal reflex mechanisms are generally normal. There is a disruption of normal reciprocal inhibition When the balance of inhibition and excitation in the basal ganglia and motor cortex is upset, the symptoms and signs of rigidity muscles and involuntary movements supervene along with abnormalities of posture and associated activity. However, our current understanding of basal ganglia pathophysiology does not provide an adequate explanation for the two other cardinal features of Parkinson’s disorder, namely, rigidity and tremor.
Several factors may contribute to rigidity muscles of which some include criteria –
- the inability of the patient to relax and completely eliminate activity in all muscles
- increased stiffness due to altered viscoelastic properties of all muscles
- abnormal co-activation of agonist-antagonist muscle groups
- increased stretch reflexes
- decreased dopamine levels
Types of Rigidity
The rigidity of Parkinson’s disorder may be characterized as either “lead pipe rigidity” or “cogwheel. rigidity”

- Cogwheel Rigidity – Refers to a hypertonic state with superimposed ratchet-like jerkiness and is generally seen in upper extremity movements (e.g., wrist/elbow flexion and extension). The cogwheel type of rigidity is a combination of lead-pipe rigidity with tremor (shake).
- Lead Pipe Rigidity – Refers to hypertonic state throughout the ROM i.e simultaneous co-contraction of agonists and antagonists and this is reflected in an immediate resistance(load) to a reversal of the direction of movement about a joint area.

Difference Between Spasticity and Rigidity
- Spasticity generally occurs only during muscle stretch (i.e., not at rest) and is usually accompanied by increased tendon reflexes and Babinski’s sign response. There is generally a difference between resistance in one direction of movement as compared to the opposite direction and some patients may represent with Clasp-Knife phenomenon (sudden release at end ROM)
- In rigidity, muscle tone is increased even at rest and is usually present during passive range of motion(ROM) in all directions across individual joints. The plantar reflex and tendon reflexes are generally normal. There is an absence of synergy.
What is the Cause Of Rigidity?
- Muscle rigidity is often triggered by stress.
- Polymyalgia rheumatica is a common condition that causes pain and stiffness in older adults.
- Unexplained weight loss and fatigue.
- In Parkinsonism pt. Decreased dopamine levels are thought to disrupt the balance between the muscles which extend and relax for each movement.
What Are The Symptoms Present in Rigidity Muscles?
- Stiff and/or inflexible muscles.
- Pain and muscle cramps.
- Difficulty turning when walking activity, turning in bed, and getting out of a chair or bed.
- The combination of tremor and increased tone is considered to be at the origin of cogwheel rigidity.
- Rigidity may be associated with joint pain.
Examination
- The observer should grasp the hand of the patent above the wrist with one hand and keep it fixed. With another hand, he holds the fingers and the palm and also slowly rotates along the long axis of the hand. If there is rigidity, the examiner will experience resistance during the activity. if the cogwheel phenomenon is positive, the observer will experience an interruption or repeated catch during the activity, and if present throughout without any disturbance or change with respect to velocity, it is lead-pipe rigidity. usually in the case of idiopathic Parkinson’s disorder, only unilateral rigidity is seen which can be compared during the examination with the contralateral side.
Treatment of Rigidity
Medical treatment
- Treatment of Parkinson’s disorder with levodopa (L-Dopa) in these various combinations is extremely helpful in reducing bradykinesia and rigidity.
- Deep Brain Stimulation in Globus pallidus stimulation and Sub thalamic nucleus stimulation has been demonstrated to improve rigidity.
Physiotherapy treatment of Rigidity
- For most patients, treatment proceeds better if rigidity is reduced early in the treatment session. accordingly, movement therapy interventions appear to have further lasting effects when the treatment is performed during the “on” phase of a medication cycle.
- Relaxation methods appear to be effective in reducing rigidity, including gentle, slow rocking, rotation of the extremities and trunk, and the use of yoga activity. In cases with Parkinson’s disorder, relaxation may be better achieved in the sitting or standing positions because rigidity may increase in the supine position. Since the proximal muscles are frequently more included than the distal group of muscles, relaxation may be easier to achieve by following a distal-to-proximal progression.
- Rhythmic Exercises are shown to decrease rigidity Eg. Clapping hands and making circles with hands or feet.
- Apply a warm compress or heating pad to the affected muscle to help relax the rigid muscle area.
- Gently stretch your stiff muscle to help relax muscles.
- Avoid strenuous activity that may trigger the muscle to become rigid again.
Relaxation & Stretching exercise :

- Gentle rocking exercise, rotational exercise in slow & rhythmic patterns.
- Rhythmic initiation method in which movement progresses from passive to active assisted and active movement.
- In supine: slow side to side head rotation activity: In hooking: lower trunk rotation activity.
- In side lying: upper and lower trunk rotation.
Balance training
- Develop high-level eccentric strength dynamic neuromuscular efficiency and reactive joint stabilization.

Balance training programs aim to:
- Strengthen balance control in every movement leading to improved fall-related self-efficacy, reduced fear of falling, and increased walking speed
- Improve physical function
- Improve the quality of life
Gait Training
- The exercises involve improving motion in your lower extremity joints(hip, knee, ankle), improving strength and balance, and mimicking the repetitive nature of your legs that occur while walking activity.
Gait Training Exercise

- Walking on a treadmill.
- Lifting your legs.
- Sitting down.
- Standing up.
- Stepping over objects.




6 Comments