

Shoulder Pain: Physiotherapy Treatment
Table of Contents
What is a Shoulder Pain?
Shoulder pain may arise from the shoulder joint itself or from any of the many surrounding muscles, ligaments, or tendons.
Shoulder pain that comes from the joint usually worsens with activities or movement of your arm or shoulder. Referred shoulder pain usually doesn’t worsen when you move your shoulder.
Shoulder Pain diagnosis is required for Proper medical and Physiotherapy treatment, for that various Physical test and X-ray/MRI is required. Physiotherapy treatment and exercise is important for reducing pain and mobility of joints.
ANATOMY OF SHOULDER :
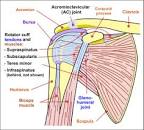
Shoulder joint is made up of three bones: the clavicle (collarbone), the scapula (shoulder blade), and the humerus (upper arm bone) as well as associated muscles, ligaments and tendons. The articulations between the bones of the shoulder make up the shoulder joints.
The shoulder joint, also known as the glenohumeral joint, is the major joint of the shoulder, but can more broadly include the acromioclavicular joint. In human anatomy, the shoulder joint comprises the part of the body where the humerus attaches to the scapula, and the head sits in the glenoid cavity. The shoulder is the group of structures in the region of the joint.
The shoulder joint is the main joint of the shoulder. It is a ball and socket joint that allows the arm to rotate in a circular fashion or to hinge out and up away from the body. The joint capsule is a soft tissue envelope that encircles the glenohumeral joint and attaches to the scapula, humerus, and head of the biceps. It is lined by a thin, smooth synovial membrane. The rotator cuff is a group of four muscles that surround the shoulder joint and contribute to the shoulder’s stability. The muscles of the rotator cuff are supraspinatus, subscapularis, infraspinatus, and teres minor. The cuff adheres to the glenohumeral capsule and attaches to the humeral head.
SIGNS & SYMPTOMS OF SHOULDER PAIN :
Common Sign And Symptoms Of Shoulder Pain Are :
- Weakness
- Inability to carry objects or use the arm
- An injury that causes deformity of the joint
- Shoulder pain that occurs at night or while resting
- Shoulder pain that persists beyond a few days
- Inability to raise the arm
- Swelling or significant bruising around the joint or arm
- Signs of an infection, including fever, skin redness, and warmth
- dull ache deep in the shoulder
- Make it difficult to comb your hair or reach behind your back. Abnormal sensations (e.g., numbness, tingling, coolness)
Causes of Shoulder Pain :
Rotator cuff tendonitis: A rotator cuff is a group of four muscles tasked with supporting and moving the shoulder. The tendons attach to the arm bone in an area underneath the bony prominence of the shoulder blade. Rotator cuff tendonitis can become pinched under this bone, which causes inflammation and soreness.
Biceps tendonitis: The biceps tendon attaches your biceps muscle in the upper arm to the front of the shoulder. This tendon can become pinched due to the bony anatomy of the shoulder blade or by ligaments that attach to the collarbone and shoulder blade.
Bursitis: Shoulder bursitis occurs when the bursa, a fluid-filled sac that enables body structures to glide smoothly over one another, becomes pinched. There is a bursa between the humerus bone and the shoulder blade.
Frozen shoulder: Also called adhesive capsulitis, frozen shoulder is a condition where the shoulder becomes painful and gradually loses motion due to lack of use, a worsening rheumatic disease, a lack of fluid to help the shoulder move, or bands of tissue that grow in the joint and restrict motion.
DIFFERENTIAL DIAGNOSIS :
> Condition
1. Impingement (tendinopathy, bursitis, PASTA)
Age usually 35-55; if younger and really looks like impingement, think instability
Overhead work or play (tennis, pitching)
Pain rolling on the shoulder in bed/ night pain. Weakness may be due to pain or torn tendon
2. rotator cuff tears
Age is usually a bit older than impingement
Pain rolling on the shoulder in bed/night pain
Weakness
Lateral arm pain, near deltoid insertion, but does not radiate below elbow
3. Suprascapular neuropathy
Presents like impingement
Constant, unrelenting pain
EMG needed
4. Multi-directional instability
dislocation, subluxation
Other joints lax
May present with impingement symptoms
5. Uni-directional instability – anterior
dislocation with or without the need for manual reduction
Usually younger patients
Pain in abduction/external rotation with Bankart lesion
6. Uni-directional Instability – Posterior
Posterior shoulder pain
May be seen with seizures/ electrocution
Pain with adduction and internal rotation
7. Labral/SLAP tears
repetitive trauma (throwing motion, overhead athletes)
May be associated with instability of the glenohumeral joint
8. Paralabral cyst
Weakness in external rotation may be present
Atrophy of infraspinatus
9. Biceps tendinopathy
Anterior shoulder pain
May also have pain with supination
Tenderness to palpation over the tendon in the bicipital groove
Popeye deformity
May be associated with subscapularis tears
10. AC arthropathy (including old fractures)
AC separation or distal clavicle fx
Weight lifter
11. AC instability
Anterior shoulder pain after a direct fall or contusion to the shoulder
May have posterior subluxation with cross-body adduction
12. Long thoracic nerve palsy
Weakness, diffuse shoulder pain
May be present after a viral illness
Winging on wall-pushup
13. Bone tumor
Pain can be at rest
14. Radiculopathy
Radiating pain, respecting dermatomal borders
Decreased/painful range of motion of the neck
Sensory disturbance along a dermatome
Radiation below elbow
15. Lung cancer
a smoking history should be enough, but too many people smoke for that to be useful. Chronic cough, weight loss, and cachexia may be more specific. Apical tumor is seen on an x-ray of the shoulder
DIAGNOSIS :
> X-ray :
An x-ray of the shoulder can detect whether or not there are any injuries to the bones that make up your shoulder joint, as well as look for subtler clues like bone spurs that could suggest a diagnosis of osteoarthritis.
>Ultrasound
Ultrasounds are typically used to investigate the rotator cuff tendon for inflammation, tears, or rupture. While it can be a helpful tool to use and can provide clues to identify the source of your pain, a diagnosis can’t be made using the ultrasound alone.
If an ultrasound is ordered, then an X-ray will also be arranged. Both tests together will provide more complete information about the state of the joints and the tendon.
> MRI :
An MRI (magnetic resonance imaging) of the shoulder can provide detailed images of the tendons, ligaments, and muscles that surround the shoulder joint. For instance, an MRI can provide information about the location, size, and even relative age of a rotator cuff tear.
MEDICAL TREATMENT :
> nonsteroidal anti-inflammatory drugs (NSAID), such as ibuprofen or naproxen, to reduce inflammation and pain.
> Corticosteroid injections to relieve the pain of a shoulder sprain, strain, or tear. Usually, doctors recommend an injection only after other medications have failed to provide relief.
SURGERY OF SHOULDER PAIN :
- Arthroscopy :
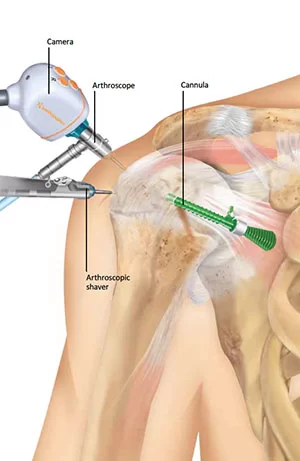
Your surgeon will first inject fluid into the shoulder to inflate the joint. This makes it easier to see all the structures of your shoulder through the arthroscope. Then your surgeon will make a small puncture in your shoulder (about the size of a buttonhole) for the arthroscope. Fluid flows through the arthroscope to keep the view clear and control any bleeding. Images from the arthroscope are projected on
the video screen showing your surgeon the inside of your shoulder and any damage. Once the problem is clearly identified, your surgeon will insert other small instruments through separate incisions to repair it. Specialized instruments are used for tasks like shaving, cutting, grasping, suture passing, and knot tying. In many cases, special devices are used to anchor stitches into bone.
FOR:- Impingement Syndrome
SLAP Repair
Shoulder Dislocation
Frozen Shoulder
2. Rotator Cuff Repairs: A large incision is made in your shoulder, then your shoulder muscle is detached so the surgeon has direct access to your tendon. This is helpful if your tendon or shoulder joint needs to be replaced. Both of these surgeries can be done under general anesthesia, which allows you to sleep through the whole thing. They can also be done with a “regional block,” which allows you to stay awake
while your arm and shoulder stay numb.
3. Acromioclavicular (AC) Joint Repairs: A transverse incision is made over the AC joint. The capsule is opened longitudinally and the dislocation is inspected. An excision of the distal clavicle of approximately 7 mm is performed and the acromion is roughened up. Two 4 mm drill holes are made in the clavicle and acromion, about 1 cm away from the AC joint. Loop PDS is passed down through the superior
aspect of the posterior hole in the acromion and retrieved in the AC joint. The loop PDS is then passed down through the superior aspect of the posterior hole in the clavicle and retrieved underneath the clavicle. It is then passed up through the inferior aspect of the anterior hole in the clavicle and brought out to the superior surface of the clavicle. Finally, the PDS is passed down through the AC joint, through the inferior aspect of the anterior hole in the acromion, and brought out of the superior aspect of this hole. This loop of PDS connects all four drill holes. The PDS is used as a shuttle for four strands of Ultrabraid (doubled back of themselves) and the palmaris graft. Overall eight strands of Ultrabraid and the tendon graft, link each drill hole. The sutures are tied and the graft is sutured to itself on the superior aspect of the
acromion Additional ties of Ultrabraid can be performed to increase tension on the joint as necessary. the capsule is closed with absorbable sutures, and the fat and skin closed in the standard fashion and the arm is placed in a poly sling.
4. Shoulder Replacement: In shoulder replacement surgery, the damaged parts of the shoulder are removed and replaced with artificial components, called a prosthesis. The treatment options are either replacement of just the head of the humerus bone (ball), or replacement of both the ball and the socket (glenoid).
5. Biceps Tendon Surgery: a surgeon inserts a special type of screw or anchoring device into the upper part of the humerus (the upper arm bone). The surgeon then clips off the end of the long head of the biceps, and sews the remaining portion of the tendon onto the screw or anchoring device so that it’s reattached to the humerus instead of the glenoid. Biceps tenodesis is performed under general anesthesia.
This procedure may be done through a small, open incision.
PHYSIOTHERAPY TREATMENT FOR SHOULDER PAIN
Heat therapy :
Heat therapy in the form of hot packs, heating pads, whirlpools, etc. can also be used in physical therapy in order to reduce pain, decrease resulting stiffness and gently increase the range of motion in dislocated shoulder patients.
Transcutaneous electrical nerve stimulation (TENS) :
TENS is another treatment modality that is a great choice for pain management. By blocking nerve impulses from the brain, TENS is able to quickly reduce acute pain associated with a dislocated shoulder.
TENS is another treatment modality that is a great choice for pain management. By blocking nerve impulses from the brain, TENS is able to quickly reduce acute pain associated with a dislocated shoulder.
Cold Pack for Shoulder Pain :
Cold Pack helps reduce both the pain and swelling a patient may experience as a result of a shoulder dislocation.
EXERCISE THERAPY FOR SHOULDER PAIN :
Pendulum Exercise :

To do the pendulum exercise, start by leaning over and supporting your non-injured arm with a table or chair. Allow the sore arm to dangle straight down and then draw circles in the air. The circles should start out small but gradually grow, and you should also reverse direction periodically. Repeat this exercise 5 to 10 times throughout the day.
Arm across the chest :
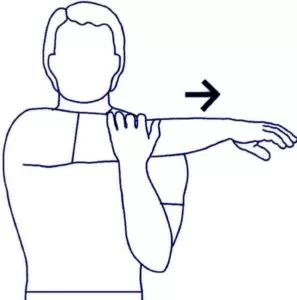
To do this stretch, hold your right hand out in front of your body, keeping it near the waist. Then reach the left hand behind the elbow while pulling the right arm to the left and across the chest. Lower the arm until the pain lessens. Hold in this position for 30 to 50 seconds and then release. Repeat this stretch 3 to 5 times.
SHOULDER STRETCH :

Stand and raise your shoulders.
Hold for 5 seconds.
Squeeze your shoulder blades back and together and hold for 5 seconds.
Pull your shoulder blades downward and hold for 5 seconds.
Relax and repeat 10 times.
DOOR PRESS :
A) Stand in a doorway with your elbow bent at a right angle and the back of your wrist against the door
frame.
Try to push your arm outwards against the door frame.
Hold for 5 seconds.
Do 3 sets of 10 repetitions on each side.
b) Use your other arm and, still with your elbow at a right angle, push your palm towards the door frame.
Hold for 5 seconds.
Do 3 sets of 10 repetitions on each side.
Side-lying external rotation :
Lie down on the side opposite your injured arm.
Bend the elbow of your injured arm to 90 degrees and rest the elbow on your side. Your forearm should
rest across your abdomen.
Hold a light dumbbell in the injured side’s hand and, keeping your elbow against your side, slowly raise
the dumbbell toward the ceiling. Stop rotating your arm if you feel the strain.
Hold the dumbbell up for a few seconds before returning to the start position with your arm down.
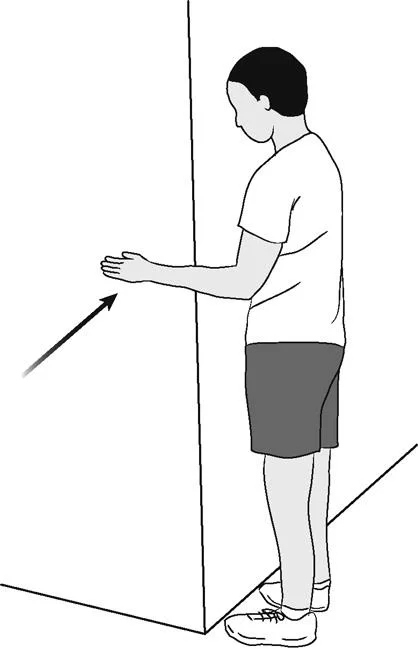
Wall Push-Ups :

Stand facing a wall with your hands on the wall shoulder-width apart. Slowly perform a push-up, lowering your chest toward the wall slowly, then pressing back. Elbows should angle behind you, not point straight out to the side.
Repeat 3 sets of 10 up to 3 times per day. Increase reps to 20 when a set of 10 becomes easy.
DO’S & DON’TS FOR SHOULDER PAIN :
- DO lie on your pain-free side. Place a pillow close to your tummy and rest your arm on it.
- DO elevate your shoulder by keeping the elbow supported during sitting and driving.
- DO use ice 20-30 minutes before bed.
- DON’T lift with your palms down.
- DON’T sit for more than 20-minute durations.
- DON’T push or pull anything when your hands are not visible.
- DON’T aggressively stretch or strengthen without your doctor or physiotherapist’s approval.


25 Comments