

Proprioceptive Neuromuscular Facilitation (PNF)
Table of Contents
INTRODUCTION
Flexibility is key for athletes and non-athletes alike. It allows you to move freely and comfortably in your daily life, and can also help prevent injury during exercise. One of the best ways to increase your flexibility is by stretching. However, research suggests that not all stretching techniques are created equal. Proprioceptive neuromuscular facilitation (PNF) stretching relies on reflexes to produce deeper stretches that increase flexibility.
Proprioceptive Neuromuscular Facilitation (PNF) is a more advanced form of flexibility training that involves both the stretching and contraction of the muscle group being targeted.
According to the International PNF Association, PNF stretching was developed by Dr. Herman Kabat in the 1940s as a means to treat neuromuscular conditions including polio and multiple sclerosis.
PNF stretching was originally developed as a form of rehabilitation, and to that effect, it is very effective. It is also excellent for targeting specific muscle groups, and as well as increasing flexibility, it also improves muscular strength.
PRECAUTION
Certain precautions need to be taken when performing PNF stretches as they can put added stress on the targeted muscle group, which can increase the risk of soft tissue injury. To help reduce this risk, it is important to include a conditioning phase before a maximum or intense effort is used.
Also, before undertaking any form of stretching it is vitally important that a thorough warm-up be completed. Warming up prior to stretching does a number of beneficial things, but primarily its purpose is to prepare the body and mind for more strenuous activity. One of the ways it achieves this is by helping to increase the body’s core temperature while also increasing the body’s muscle temperature. This is essential to ensure the maximum benefit is gained from your stretching. Click here for a detailed explanation of how, why, and when to perform your warm-up.
EFFECT OF PNF
While there are multiple PNF stretching techniques, all of them rely on stretching a muscle to its limit. Doing this triggers the inverse myotatic reflex, a protective reflex that calms the muscle to prevent injury.
“PNF causes the brain to go ‘I don’t want that muscle to tear’ and sends a message to let the muscle relax a little more than it would normally,” says fasciologist Ashley Black.
PNF is a stretching technique utilized to increase ROM and flexibility. PNF increases ROM by increasing the length of the muscle and increasing neuromuscular efficiency.
PNF TECHNIQUES
Revarsal of Antagonists:
A group of techniques that allow for agonist contraction followed by antagonist contraction without pause or relaxation.
- Dynamic Reversals (Slow Reversals): Utilizes isotonic contractions of first agonists, then antagonists performed against resistance. Contraction of the stronger pattern is selected first with progression to the weaker pattern. The limb is moved through a full range of motion.
Indications Impaired strength and coordination between agonist and antagonist, limitations in range of motion, fatigue. - Stabilizing Reversals: Utilizes alternating isotonic contractions of first agonists, then antagonists against resistance, allowing only a very limited range of motion.
Indications Impaired strength, stability and balance, coordination.
Rhythmic Stabilization (RS):
Utilizes alternating isometric contractions of first agonists, then antagonists against resistance; no motion is allowed.
Indications Impaired strength and coordination, limitations in ROM; impaired stabilization control and balance.
Repeated Contractions, RC (Repeated stretch):
Repeated isotonic contractions from the lengthened range, induced by quick stretches and enhanced by resistance; are performed through the range or part of the range at a point of weakness. The technique is repeated (i.e., three or four stretches) during one pattern or until contraction weakens.
Indications Impaired strength, initiation of movement, fatigue, and limitation in active ROM.
Rhythmic Initiation (RI):
Voluntary relaxation is followed by passive movements progressing to active assisted and active resisted movements to finally active movements. Verbal commands are used to set the speed and rhythm of the movements. Light tracking is used during the resistive phase to facilitate movement.
Indications Inability to relax, hypertonicity (spasticity, rigidity); difficulty initiating movement; motor planning deficits (apraxia or dyspraxia); motor learning deficits; communication deficits (aphasia).
Hold-relax
One PNF technique that Black says can trigger the reflex is commonly called “hold-relax.” This involves:
Putting a muscle in a stretched position and holding for a few seconds.
Contracting the muscle without moving (also called isometric), such as pushing gently against the stretch without actually moving. This is when the reflex is triggered and there is a “6- to 10-second window of opportunity for a beyond ‘normal’ stretch,” Black says.
Relaxing the stretch, and then stretching again while exhaling. This second stretch should be deeper than the first.
Contract-relax
Another common PNF technique is the contract-relax stretch. It is almost identical to hold-relax, except that instead of contracting the muscle without moving, the muscle is contracted while moving. This is sometimes called isotonic stretching.
For example, in a hamstring stretch, this could mean a trainer provides resistance as an athlete contracts the muscle and pushes the leg down to the floor.
Hold-relax-contract
A third technique, hold-relax-contract, is similar to hold-relax, except that after pushing against the stretch, instead of relaxing into a passive stretch, the athlete actively pushes into the stretch.
For example, in a hamstring stretch, this could mean engaging the muscles to raise the leg further, as the trainer pushes in the same direction.
Regardless of technique, PNF stretching can be used on most muscles in the body, according to Black. Stretches can also be modified so you can do them alone or with a partner.
Rhythmic Rotation
Relaxation is achieved with slow, repeated rotation of a limb at a point where limitation is noticed. As muscles relax the limb is slowly and gently moved into the range. As a new tension is felt, RRo is repeated. The patient can use active movements (voluntary efforts) for RRo or the therapist can perform RRo passively. Voluntary relaxation when possible is important.
Indications Relaxation of excess tension in the muscles (hypertonia) combined with PROM of the range-limiting muscles.
To that end, PNF Techniques have broad applications in treating people with neurologic and musculoskeletal conditions, most frequently in rehabilitating the knee, shoulder, hip and ankle.
PNF PATTERN
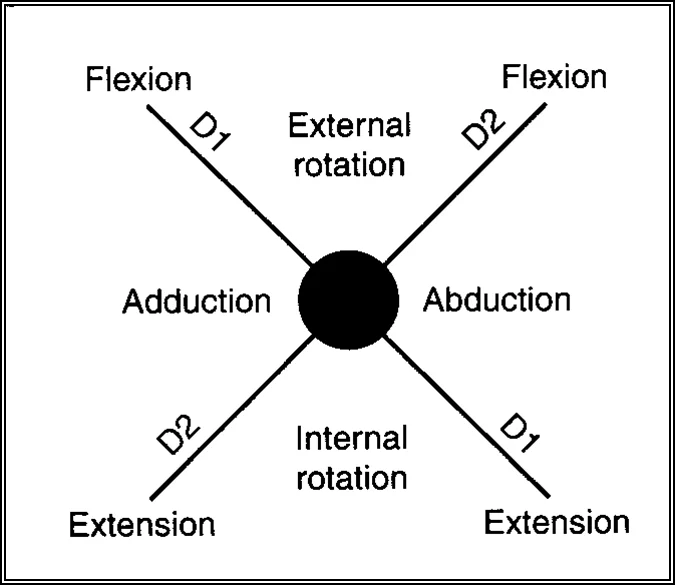
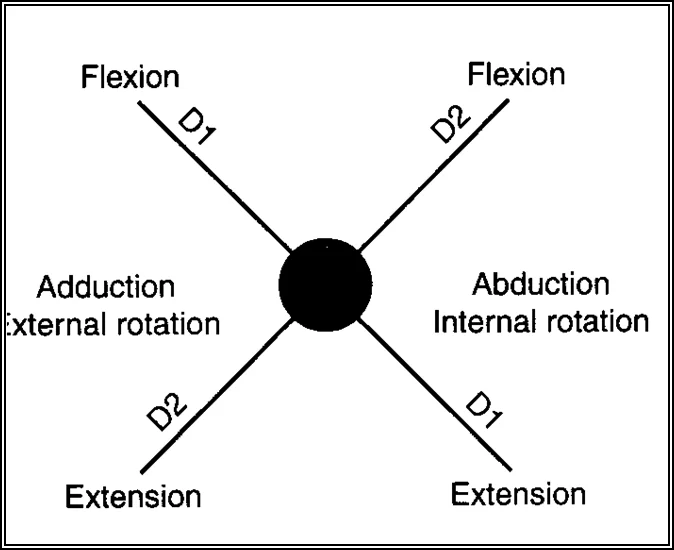
- The PNF exercise patterns involve three components: flexion extension, abduction-adduction, and internal-external rotation.
- The patterns mimic a diagonal rotation of the upper extremity, lower extremity, upper trunk, and neck.
- The pattern activates muscle groups in the lengthened or stretched positions.
- The upper and lower extremities each have two patterns: D1 and D2 motions targeting flexion and extension.
- The patterns are used to improve the range of motion at the joint as well as introduce resistance training. This will help improve the patient’s strength.
Upper Extremity
D1 Flexion

Starting Position
Shoulder extended, abducted, and internally rotated
Forearm pronated
Wrist ulnarly deviated
Fingers extended
Hand Position
Hand placed in patient’s palm so that patient can grip and flex wrist to the radial side
hand on the Anterior-medial surface of the patient’s arm just above the elbow.
Movements to End Position
Shoulder flexed, adducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers flexed
D1 Extension

Starting Position
Shoulder flexed, adducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers flexed
Hand Position
Hand over dorsal-ulnar aspect of the patient’s hand
hand on the posterior-lateral surface of the patient’s arm just above the elbow
Movement to Ending Position
Shoulder extended, abducted, and internally rotated
Forearm pronated
Wrist ulnarly deviated
Fingers extended
D2 Flexion

Starting Position
Shoulder extended, adducted, and internally rotated
Forearm pronated
Wrist ulnarly deviated
Fingers flexed
Hand Position
Hand over dorsal-ulnar aspect of the patient’s hand
Hand on anterior-lateral surface of the patient’s arm just above elbow
Movements to End Position
Shoulder flexed, abducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers extended
D2 Extension

Starting Position
Shoulder flexed, abducted, and externally rotated
Forearm supinated
Wrist radially deviated
Fingers extended
Hand Position
The hand is placed in the patient’s palm so that the patient can grip and flex the wrist to the ulnar side
Hand on posterior-medial surface of the patient’s arm just above the elbow
Moving to the Ending Position
Shoulder extended, adducted, and internally rotated
Forearm pronated
Wrist ulnarly deviated
Fingers flexed
Lower Extremity
D1 Flexion

Starting Position
Hip extended, abducted, and internally rotated
Ankle plantarflexed
Foot everted
Toes flexed
Hand Position
Hand on distal anterior-medial aspect of the thigh
Hand on the medial aspect of the dorsal surface of foot
Movements to Ending Position
Hip flexed, adducted, and externally rotated
Ankle dorsiflexed
Foot inverted
Toes extended
D1 Extension

Starting Position
Hip flexed, adducted, and externally rotated
Ankle dorsiflexed
Foot inverted
Toes extended
Hand Position
Hand on distal posterior-lateral thigh
Hand on the lateral aspect of the plantar surface of the foot
Movements to Ending Position
Hip extended, abducted, and internally rotated
Ankle plantarflexed
Foot everted
Toes flexed
D2 Flexion

Starting Position
Hip extended, adducted, and externally rotated
Ankle plantarflexed
Foot inverted
Toes flexed
Hand Position
Hand on distal anterior-lateral thigh
Hand on lateral aspect of dorsal surface of the foot
Movements to Ending Position
Hip flexed, abducted, and internally rotated
Ankle dorsiflexed
Foot everted
Toes Extended
D2 Extension

Starting Position
Hip flexed, abducted, and internally rotated
Ankle dorsiflexed
Foot everted
Toes Entended
Hand Position
Hand on distal posterior-medial thigh (wrapped around posterior aspect of femur)
Hand on medial aspect of plantar surface of the ball of the foot
Movements to Ending Position
Hip extended, adducted, and externally rotated
Ankle Plantarflexed
Foot inverted
Toes flexed
FAQ
3 PNF techniques are:
Contract-Relax Method.
Agonist-Contract Method.
Contract-Relax-Agonist-Contract Method.
PNF techniques:
Stretching a muscle and holding it there for a short while (also known as a passive stretch).
Isometric contraction is defined as contracting a muscle without moving; an example of this would be slowly applying pressure to a stretch without moving.
Exhaling as you relax the stretch and then re-extend it.
For instance, to stretch your hamstrings PNF with a partner: With one leg stretched toward the ceiling, lie on your back. Stretch: Press your leg gently toward your face, and have your partner move it into a static stretch. Give the static stretch ten or so seconds to hold.
Basic Principles of PNF:
Manual pressure is the act of moving hands in the desired direction. Verbal Stimulation: To elicit the intended movement, use the appropriate language. “Pull – Push.”
PNF patterning, which is divided into D1 (Diagonal 1) and D2 (Diagonal 2) patterns, is used for the upper and lower limbs. The elbow, wrist, fingers, and shoulder are all included in the upper extremity pattern. Comparably, the hip, knee, ankle, and toes are included in the lower extremity pattern.
Your range of motion can be enhanced by the stretching method known as proprioceptive neuromuscular facilitation (PNF). PNF is a common tool used by therapists to aid patients in regaining range of motion following surgery or injury. Athletes can utilize it, though, to increase their flexibility.


I love PNF and practice it every day.
I have a question:
We know that most proprioceptors are placed in C0-C3, in the foot soles and in the costovertebral joints.
But what about hip, sholuder, knee, elbow etc.
in my point of view there must be more proprioceptors in the hip than in the knee and also more proprioceptors around the shoulder than the elbow because of the amount of muscles and a greater need for stabilisation