
Muscle Energy Technique (MET)
Table of Contents
What is a Muscle Energy Technique (MET)?
Muscle Energy Technique (MET) was developed by Fred L. Mitchell, Sr., D. O. This technique is classified as an active technique in which the patient voluntarily uses his muscles from a precisely controlled position in a specific direction, against a distinctly executed counter-force.
MET may be used to lengthen the shortened or spastic muscle, to strengthen weakened muscles, to reduce localized edema, or to mobilize restricted joint motion.
Definition of Muscle Energy Technique (MET)
Muscle Energy Techniques describes a broad class of manual therapy techniques directed at improving musculoskeletal function or joint function, and improving pain. METs are commonly used by manual therapists.
Types of MET:
There are mainly 2 types of MET :
- Autogenic Inhibition MET
- Post Isometric Relaxation (PIR)
- Post Facilitation Stretching (PFS)
2. Reciprocal Inhibition MET
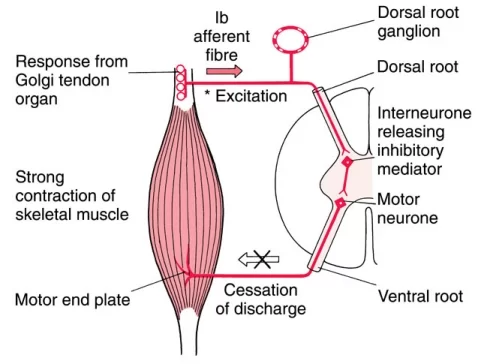
1) AUTOGENIC INHIBITION:
-Autogenic inhibition reflex is a sudden relaxation of muscle upon the development of high tension. It is a self-induced, inhibitory, negative
feedback prolong lengthen reaction against tear muscles. Golgi tendon organs are receptors responsible for that.
Autogenic inhibition (historically known as the inverse myotatic reflex or autogenetic inhibition) shows a decrease in the excitability of a contracting or stretched muscle that in the past has been merely ascribed to the increased inhibitory input arising from Golgi tendon organs (GTOs) within the same muscle.
The reduced efferent (motor) send to the muscle through autogenic inhibition is a factor that will help muscle elongation.
Golgi tendon organs are receptors responsible for that Autogenic inhibition (historically known as the inverse myotatic reflex or autogenetic inhibition) shows a decrease in the excitability of a contracting or stretched muscle that in the past has been merely ascribed to the increased inhibitory input arising from Golgi tendon organs (GTOs) within the same muscle.
The reduced efferent (motor) send to the muscle through autogenic inhibition is a factor that will help muscle elongation.
Ex. GTOs sense muscular tension within muscles when they contract or are stretched. When the GTO is activated during contraction, it causes inhibition of the contraction (autogenic inhibition), which is an automatic reflex. Static stretching is one example of how muscle tension signals a GTO response.
- POST ISOMETRIC RELAXATION (PIR):- Post Isometric Relaxation is a technique developed by Karel Lewitt. Post Isometric Relaxation(PIR) is the effect of the decrease in muscle tone in a single or group of muscles, after a brief period of submaximal isometric contraction of the same muscle. PIR works on the concept of autogenic inhibition.
The PIR technique is performed as follows:
After the isometric contraction, the patient is asked to relax and exhale while doing so. Following this, a gentle stretch is applied to take up the slack till the new barrier.
- POST-FACILITATION STRETCHING (PFS): Post-facilitation stretch (PFS) is a technique developed by Dr. Vladimir Janda that involves a maximal contraction of the muscle at mid-range with a rapid movement to maximal length followed by a 15-second static stretch.
The PFS technique is performed as follows: The hyper-tonic and shortened muscles are placed between a fully stretched and a fully relaxed state. The patient is asked to contract the agonist using a maximum degree of effort for 5–10 seconds while the therapist resists the patient’s force.
2) RECIPROCAL INHIBITION:
The reciprocal inhibition process recognized as when the muscle spindle, which is placed within the muscle, tummy and stretches alongside with the muscle itself.
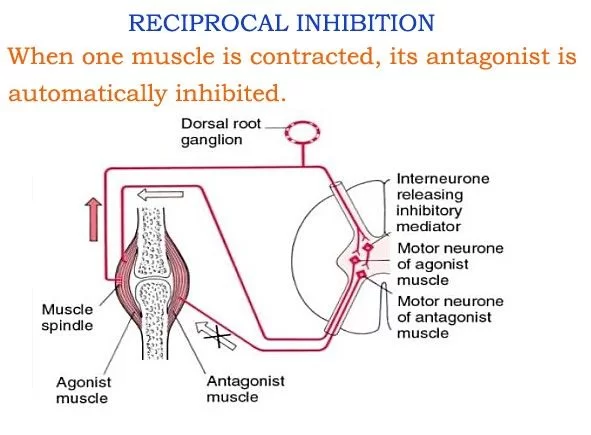
When this occurs, the muscle spindle is activated and causes a reflexive contraction in the agonist’s muscle (known as the stretch reflex) and relaxation in the antagonist’s muscle.
Reciprocal inhibition mediated via the muscle spindle Ia afferents from the antagonist’s muscle was identified and investigated in healthy subjects. The reciprocal Ia inhibition is enhanced throughout voluntary activation of the antagonist, e.g. it prevents stretch reflexes in the antagonist’s muscle as the muscle is passively stretched.
In spastic patients, in hemiplegia in addition to paraplegia, the quantity of Ia reciprocal inhibition is reduced and its regulation during (the remaining) voluntary movement is more or less eliminated.
Ex. Reciprocal inhibition is a neuromuscular reflex that inhibits opposing muscles during movement. For example, if you contract your elbow flexors (biceps) then your elbow extensors (triceps) are inhibited. This is the idea behind active stretching, and one component of PNF stretching.
- The Reciprocal Inhibition MET TECHNIQUE is performed as follows: The affected muscle is placed in a mid-range position. The patient pushes towards the restriction/barrier whereas the therapist completely resists this effort (isometric) or allows a movement towards it (isotonic).
PATHOPHYSIOLOGY:
Injury can occur as a result of trauma, accidents, overuse, strain/sprain, etc., not all of which should be treated with muscle energy. These techniques are most appropriate for the following injury patterns:
- Decreased range of motion secondary to muscular spasticity, rigidity, hypertonicity, or hypotonicity.
- Hypertonicity often follows overuse and can result in altered joint position, increased irritability, and decreased elasticity. This injury pattern is often accompanied by a non-specific muscle ache in the area of injury.
- Interneuronal injury—when dysfunction occurs at one joint-segment, the related agonist muscles are also affected. If uncorrected, the antagonistic muscles eventually become involved as well, leading to dysfunction of both muscle groups. This presents as decreased range of motion with pain and/or tenderness in the area,
MECHANISM OF ACTION:
Muscle energy is a direct and active technique; meaning it engages a restrictive barrier and requires the patient’s participation for maximal effect.
A restrictive barrier describes the limit in the range of motion that prevents the patient from being able to reach the baseline limit in his range of motion. As the patient performs an isometric contraction, the following physiologic changes occur:-
- Golgi tendon organ activation results in direct inhibition of the agonist’s muscles.
- A reflexive reciprocal inhibition occurs at the antagonistic muscles.
- As the patient relaxes, agonist and antagonist muscles remain inhibited, allowing the joint to be moved further into the restricted range of motion.
Benefits of MET:
- Restoring normal tone in hypertonic muscles
- Strengthening weak muscles
- Preparing muscle for subsequent stretching
- Improved joint mobility
USES:
- Lengthen a shortened, contractured, or spastic muscle.
- Strengthen physiologically weakened muscles.
- Reduce pain.
- Stretch the tight fascia.
- Reduce localized edema.
- Mobilize an articulation with restricted mobility.
ELEMENTS OF MET PROCEDURE:
1) Patient:- active muscle contraction.
2) Controlled joint position.
3) Controlled contraction intensity.
4) Muscle contraction in a specific direction.
5) Operator applied distinct counterforce.
INDICATIONS:
- Normalize abnormal neuromuscular relationship.
- Improve local circulation and respiratory function.
- Lengthen and normalize restricted / hypertonic muscle and fascia.
- Mobilize restricted joints.
- Movement restriction due to muscle tightness.
- Muscle hyperactivity.
- Acute injuries.
- Myofascial restrictions, muscle imbalance.
CONTRAINDICATIONS:
- Avoid in:- Fracture
~Severe sprain
~Severe strain
~Open wounds
~Severe osteoporosis
~Avulsion injury
~Metabolic bone
~Unconscious patients or those who can not or will not follow
directions.
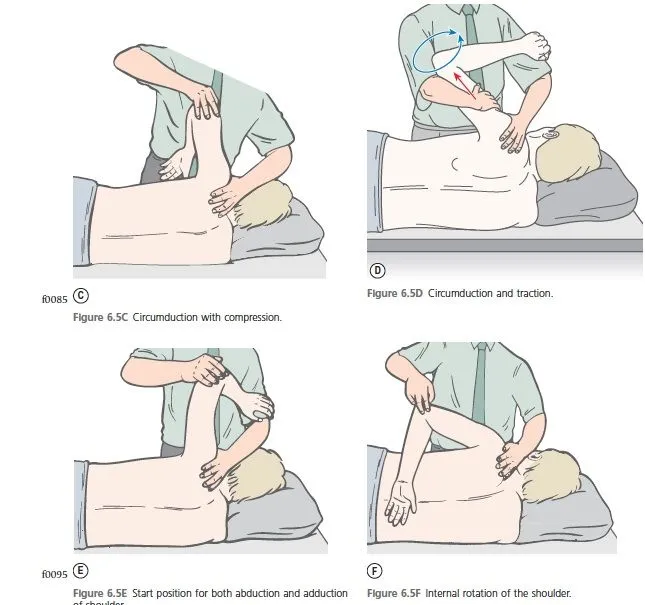
EXAMPLES OF MUSCLE ENERGY TECHNIQUE:
| Target Structure | Starting Position | Therapist’s hand 1 | Therapist’s hand 2 | Patient action |
|---|---|---|---|---|
| Psoas Major | Thomas test position: Supine on the plinth, target leg hanging off the plinth, the other leg in 90 degrees flexion the rest of the body on the plinth | Just above the knee of the plinth | Just above the knee of the leg inflection | Flexes the hip hanging off the plinth |
| ITB | Side-lying, target leg off the plinth | Over superior lateral thigh | Over superior lower leg | Abducts the hip |
| Hip External Rotators | Crook-lying | Over lateral mid-thigh | Over inferior mid-thigh | Abducts leg against the therapist |
SELF-ADMINISTERED Muscle Energy Technique (MET):
1)Hip Flexion/Hip Extension:
Patient in crook lying places foot on the contralateral knee
– Brings foot down against knee, brings a knee up against the foot
2)Hip adduction:
The patient has a ball between legs in crook lying, squeezes the ball
3)Hip external rotation:
Patient in prone with the hip and knee flexed to 90 degrees
The therapist moves the knee into internal rotation, the patient pushes against the therapist
4)Scalenes:
Patient in supine, shoulders on a pillow, head hanging off pillow
Therapist places into extension and rotation
Patient resists therapist into neutral (flexing and rotating)



4 Comments