

Golfer’s Elbow Test
Table of Contents
What is a Golfer’s Elbow Test?
The golfer’s elbow test is a simple physical examination that helps diagnose medial epicondylitis, commonly known as golfer’s elbow. This condition involves inflammation and pain in the tendons that attach to the bony bump on the inside of the elbow.
If the person experiences pain along the inside of the elbow or forearm during the resistance test, it suggests the presence of golfer’s elbow. However, it is important to note that the golfer’s elbow test is not definitive and should be combined with other diagnostic techniques, such as a thorough medical history, physical examination, and possibly imaging studies like an X-ray or MRI, for an accurate diagnosis.
If someone is experiencing persistent or severe elbow pain, it is recommended to consult a healthcare professional, such as a doctor or orthopedic specialist, for proper evaluation and diagnosis.
What is a Golfer’s Elbow?
- Golfer’s elbow (medial epicondylitis or pitcher’s elbow) is a type of tendinopathy caused by overuse or overload that affects the elbow’s medial common flexor tendon. This can occur gradually, with patients describing aching discomfort radiating from the epicondyle to the wrist. This exercise depicts the examination and therapy of golfers’ elbow and discusses the role of the interprofessional team in enhancing care for individuals suffering from this ailment. Medial epicondylitis, sometimes known as golfer’s elbow, is tendinopathy of the elbow’s medial common flexor tendon caused by stress or overuse. Pitcher’s elbow, tendinosis, or epicondylalgia may alternatively be used instead of epicondylitis.
Purpose of Golfer’s Elbow Test
The Medial Epicondylalgia “Golfer’s Elbow” Test is used to evaluate patients for medial epicondylalgia or “golfer’s elbow.”
Clinical Examination
- Tenderness from the medial epicondyle to the pronator teres and flexor carpi radialis muscles was seen on clinical examination.
- Pain might be caused by medial epicondylalgia/golfer’s elbow. A provocative special test is used to check for medial epicondylalgia in addition to discomfort.
Technique of Golfer’s Elbow Test

Passive Technique
- For this exam, the patient could be either sitting or standing.
- The therapist uses one hand to palpate the medial epicondyle and support the elbow while the other hand passively supinates the patient’s forearm and completely extends the elbow, wrist, and fingers.
- The test is considered positive if acute pain or discomfort occurs again along the medial epicondylar area.
Active Technique
- For this exam, the patient could be either sitting or standing.
- The patient flexes and pronates their wrist and forearm as the examiner resists.
- The test is considered positive if acute pain or discomfort is replicated along the medial epicondylar area.
Special Considerations
- Structure injury to the ulnar nerve, ulnar collateral nerve, or ulnar collateral ligament can also produce pain along the medial epicondylar area of the elbow.
- It is essential to evaluate each of these structures before drawing any judgments based just on this test.
Evidence
There are no current studies that demonstrate the Medial Epicondylalgia “Golfer’s Elbow” Test’s diagnostic accuracy.
Other Golfer’s Elbow Test:
- Polk’s test
- Reverse Cozen’s Test
Polk’s Test
- Polk’s test is simple to learn, carry out, and interpret test that can assist clinicians in differentiating between Lateral Epicondylitis and Medial Epicondylitis.
- It assists the physician in developing a workable diagnosis and also acts as an instructional tool for the patient, allowing them to better understand their condition and avoid actions that worsen the injury.
Clinically Relevant Anatomy
There are no current studies that demonstrate the diagnostic accuracy of the Medial Epicondylalgia “Golfer’s Elbow” Test.
Resources
Other tests to evaluate a golfer’s elbow include:
- Polk’s test
- Reverse Cozen’s Test
Polk’s test
Purpose
- Polk’s test could assist physicians in determining between Lateral Epicondylitis and Medial Epicondylitis, two of the most common causes of elbow pain.
Polk’s test is also helpful in figuring out which type of lifting should be avoided by the patient. - The Polk’s test works on a very simple mechanism. When the hand grasps an item, strain is produced on both the wrist flexors and extensors. Lifting an object increases stress on the major afflicted muscle group, causing mechanical strain at the inflamed musculotendinous attachment point.
Technique

The patient is told to lift an item weighing approximately 2.5 kg while seated and with the elbow flexed. For most tests, a properly weighted sandbag, hand weight, heavy purse, or thick book will serve.
The test is divided into two phases:
Phase 1: lateral epicondylitis diagnosis
- The patient grasps the object with the palm towards the floor (forearm pronation) and is advised to attempt to raise it up. Lateral Epicondylitis is characterized by pain in the elbow, typically in the area of the lateral epicondyle, as a result of this technique.
- In the absence of lateral epicondylitis, the patient normally executes this technique relatively easily and painlessly.
Phase 2: medial epicondylitis diagnosis
- This phase consists of the patient is in a sitting position with an elbow flexed. The patient is encouraged to grab the object with the palm up (forearm supination) and attempt to raise it. This motion causes elbow discomfort, mainly in the area of the medial epicondyle, which is symptomatic of Medial Epicondylitis.
- The patient executes this movement pretty comfortably in the absence of medial epicondylitis.
Reverse Cozen’s Test
What is Reverse Cozen’s Test?
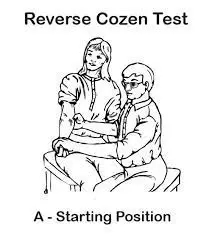
- The reverse cozen test is used to detect pain caused by disease of the common flexor tendon at its attachment to the medial epicondyle.
- Historically, it was known as Golfer’s elbow or medial epicondylitis. Most recent studies, however, propose adopting the term medial elbow tendinopathy. The reverse cozen test, on the other hand, aids in the diagnosis of the Golfer’s elbow (medial epicondylitis).
- The method for performing the Reverse Cozen’s Test
- Ask your patient to place his arm supinated.
- The examiner now stabilizes the patient’s elbow with one hand and puts his index finger over the medial epicondyle.
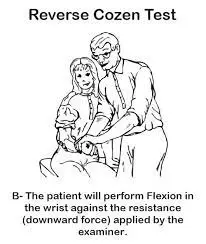
Make a fist with the patient and then flex their wrists together with a small ulnar deviation.
Now tell the patient to remain in this position. Finally, instruct the patient to practice wrist flexion against the examiner’s resistance (downward force).
Assessment of the Reverse Cozen Test
- If the test aggregates or reproduces the pain at the medial epicondyle, it is considered positive. The medial epicondyle is the origin of the forearm (common flexor tendon) and hand flexors. Acute, stabbing pain at the medial epicondyle indicates medial epicondylitis.
- It is critical to stabilize the elbow while completing this examination. A violent avoidance or pronation action, on the other hand, might aggravate a compression condition (pronator compartment syndrome) in the pronator teres muscle.
FAQ
The disorder is known as a golfer’s elbow because this tendon is pressured during a golf swing, especially if a non-overlapping (baseball-type) grip is employed; nevertheless, many people develop the condition without ever playing golf.
Golfer’s elbow, baseball elbow, suitcase elbow, and forehand tennis elbow are all names for medial epicondylitis. It is defined by discomfort on the inside (medial side) of the elbow from the elbow to the wrist. Damage to the tendons that bend the wrist towards the palm causes discomfort.
The pronator teres and the FCR are the primary muscles involved in medial epicondylitis. Palmaris longus, FDS, and FCU are less likely to be involved. The anterior medial epicondyle is the most commonly involved location in this disease.
Overuse of the forearm muscles that allow you to grab, rotate your arm, and flex your wrist is the most common cause of a golfer’s elbow. Repetitive flexing, gripping, or swinging can strain or tear tendons. With its name, this disease does not only affect golfers.
A golfer’s Elbow is a sprain or strain caused by a strain on the tendons on the inside of your elbow.
Cold therapy (such as an ice pack) might help relieve discomfort from the region that is affected if it occurs during the first 72 hours. If the pain is persistent and recurring, heat therapy (such as a heating pad) is the preferable treatment.
Combining cold and compression is the most effective strategy to address Golfer’s Elbow discomfort and inflammation. Icing (10-15 minutes) constricts the blood vessels, slowing circulation and stopping metabolic activity, reducing inflammation and discomfort.
The injury is usually caused by excessive or recurrent stress, particularly strong wrist and finger motions. Improper lifting, throwing, or striking techniques, as well as an insufficient warmup or inadequate fitness, can all lead to a golfer’s elbow.





