
FRACTURE NECK OF FEMURE: Complication, Diagnosis, Treatment
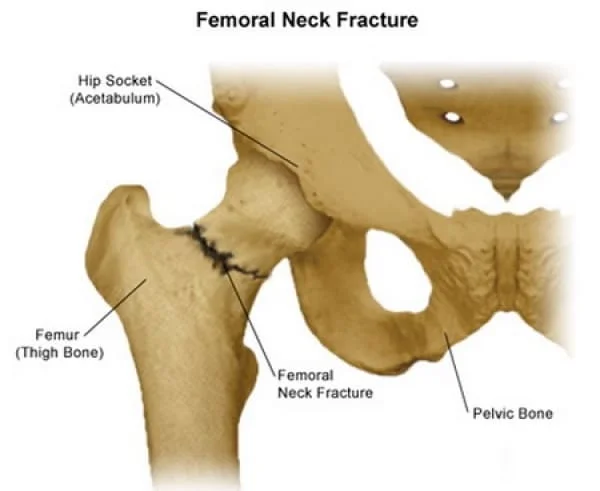
A fractured neck of femur (broken hip) is a serious injury, especially in older people. It is likely to be life changing and for some people life threatening. It occurs when the top part of the femur (leg bone) is broken, just below the ball and socket joint.
Neck of femur fractures (NOF) are common injuries sustained by older patients who are both more likely to have unsteadiness of gait and reduced bone mineral density, predisposing to fracture. Elderly osteoporotic women are at greatest risk.
Femoral neck fractures and peritrochanteric fractures are equally prevalent and make up over 90 percent of proximal femur fractures.
The femoral neck is the most common location for a hip fracture. Your hip is a ball and socket joint where your upper leg meets your pelvis. At the top of your femur (which is your thigh bone) is the femoral head. This is the “ball” that sits in the socket. Just below the femoral head is the femoral neck.
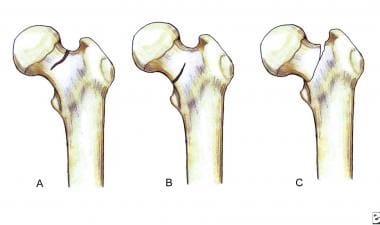
- subcapital is the femoral head and neck junction
- transcervical is the mid portion of femoral neck
- basicervical is the base of femoral neck
- Though anyone can fracture their femoral neck, it’s considerably more common in elderly adults who have poor bone density. More than 90 percentTrusted Source of these fractures occur in people older than 50. They are more common in women.
Femoral neck fractures are intracapsular fractures. The capsule is the area that contains the fluid that lubricates and nourishes the hip joint. Fractures in this area are categorized based on the location of the fracture along the femoral neck:
A femoral neck fracture can tear the blood vessels and cut off the blood supply to the femoral head. If the blood supply to the femoral head is lost, the bone tissue will die (a process called avascular necrosis), leading to the eventual collapse of the bone. Fractures that occur in places where the blood supply is not disrupted have a better chance of healing.
For these reasons, treatment for an elderly patient with displaced femoral fractures will depend upon the location of the break and the quality of the blood supply.
The standard of care for a displaced fracture where the blood supply is disrupted involves replacing the femoral head (hemiarthroplasty or total hip arthroplasty). If there’s no displacement, then surgically stabilizing the fracture with screws or other hardware may be done. However, there’s still the risk that the blood supply may be disrupted.
Table of Contents
Epidemiology
Incidence is increasing as the proportion of the elderly population in many countries increases 4. In patients aged between 65 and 99, femoral neck and intertrochanteric fractures occur with approximately the same frequency.
Pathology
Classification
- Intracapsular – either subcapital (through the junction of the head and neck) or basocervical fracture (through the base of femoral neck)
- Extracapsular – either intertrochanteric (between the two trochanters) or subtrochanteric (<5cm distal to the lesser trochanter)
Neck of femur fractures can be classified by the fracture line in relation to the joint capsule:
Femoral neck fractures are a subset of proximal femoral fractures. The femoral neck is the weakest part of the femur.
Since disruption of blood supply to the femoral head is dependent on the type of fracture and causes significant morbidity, diagnosis and classification of these fractures is important. There are three types:
- subcapital: femoral head/neck junction
- transcervical: midportion of femoral neck
- basicervical: base of femoral neck
- Most significantly, subcapital and transcervical fractures are considered intracapsular while basicervical fractures are considered extracapsular 14.
Further, severity of a subcapital fracture is graded by the Garden classification of hip fractures.
Mechanism of Injury
falls in the elderly
significant trauma (e.g. motor vehicle collisions) in younger patients
In elderly patients, the mechanism of injury various from falls directly onto the hip to a twisting mechanism in which the patient’s foot is planted and the body rotates. There is generally deficient elastic resistance in the fractured bone 8.
The mechanism in young patients is predominantly axial loading during high force trauma 9, with an abducted hip during injury causing a neck of femur fracture and an adducted hip causing a hip fracture-dislocation.
A femoral neck stress fracture causes
Trauma is the most common cause of femoral neck fractures. Being over the age of 50 or having a medical condition that weakens your bones, such as osteoporosis, increases your risk of a fracture in the femoral neck. Having bone cancer is also a risk factor.
Falls are the most common cause of femoral neck fractures in older adults. In younger people, these fractures most often result from high-energy trauma, such as a vehicle collision or fall from a great height.
Femoral neck fractures are rare in children. Along with high-energy trauma, they can also be caused by low bone mineral density, such as osteopenia or osteoporosis, or by other conditions like cerebral palsy or muscular dystrophy.
Femoral neck fracture symptoms
The most common symptom of a femoral neck fracture is pain in the groin that gets worse when you put weight on the hip or try to rotate the hip. If your bone is weakened by osteoporosis, cancer, or another medical condition, you might experience groin pain leading up to the time of the fracture.
With a femoral neck fracture, your leg may appear shorter than your uninjured leg, or your leg may be externally rotated with your foot and knee turned outward.
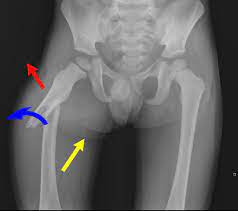
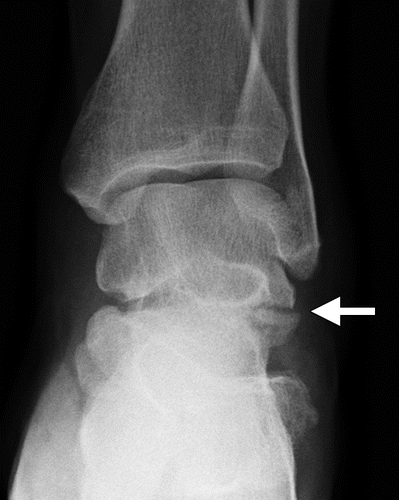
Radiographic features
Plain radiographs (sensitivity 93-98%) is the first-line investigation for suspected NOF fractures. In patients with a suspected occult NOF fracture, MRI (sensitivity 99-100%) is recommended by many institutions as the second-line test if available within 24 hours, with CT or nuclear medicine bone scan third-line 17,18. However, a recent study reports that thin-slice MDCT is as sensitive as MRI 19.
- Shenton’s line disruption: loss of contour between normally continuous line from medial edge of femoral neck and inferior edge of the superior pubic ramus
- lesser trochanter is more prominent due to external rotation of femur
- femur often positioned in flexion and external rotation (due to unopposed iliopsoas)
- asymmetry of lateral femoral neck/head
- sclerosis in fracture plane
- smudgy sclerosis from impaction
- bone trabeculae angulated
- nondisplaced fractures may be subtle on x-ray
- Report checklist
- AP pelvis and lateral hip should be viewed because pelvic fractures can mimic clinical features of hip fracture
- trace Shenton’s line
- assess for symmetry, particularly note lesser trochanter (may indicate external rotation)
- bone trabeculae
- sclerosis
- smudge
Plain radiograph
Complications
Loss of fixation. Implants that are used for internal fixation of the proximal femur are prone to failure due to the large bending loads that are present in the proximal femur and the poor bone quality that is usually associated with fracture. Many displaced fractures are unstable, with posterior and medial comminution leading to loss of a stable medial buttress. The implant may cut out of the superior femoral neck as the fracture settles into varus displacement, break at the site of the fracture, or, in the case of a side-plate device, pull out from the femoral shaft. Technical problems that may lead to failure include poor screw position, placement of screws with threads that cross the fracture site, or imperfect fracture reduction. Failure of internal fixation of a femoral neck fracture with either multiple pins or a sliding hip screw is most dependent on bone quality and screw placement . Swiontkowski and colleagues[53] demonstrated a lack of benefit with more than 3 pins and that bone density is a useful predictor of the success of fixation.
The treatment of failed osteosynthesis of the femoral neck depends on the timing of failure, the mode of failure, and the patient’s general condition and activity level. Repeat fixation may be considered in cases of early failure if bone stock is adequate. Often, a valgus osteotomy is necessary to restore the correct mechanical axis of the femoral neck. Conversion to an arthroplasty is required if osteonecrosis ensues or because of poor bone quality. Long-stem devices should be used to ensure that the tip of the stem is distal to the screw holes in the lateral femoral cortex.
Nonunion. Delayed or nonunion of a femoral neck fracture occurs in 15% to 40% of cases and is often manifested by continued pain with weight bearing beyond 3 months of fixation. Nonunion generally becomes apparent within 1 year. The risk is greater with displaced fractures.
The variability in the incidence of nonunion in different series may be explained by fracture type and by the authors’ methods of reduction and fixation technique. Madsen and colleagues,for example, observed that the union rate of displaced femoral neck fractures was higher after fixation with 4 cancellous screws (84%) than with a sliding screw plate (64%). Nonunion is associated with pin migration, both of which were reported to occur only in displaced fracture patterns. Valgus reduction appeared to protect against pin migration In a review of 141 patients who underwent osteosynthesis of femoral neck fractures with 6.5-mm AO screws, Hammer reported that the incidence of nonunion was correlated with the Garden classification: 1% for Garden I fractures and more than 25% in Garden III and IV fractures. Irrespective of the Garden classification, a vertical fracture orientation resulted in a 40% incidence of nonunion.
Nonunion may or may not be accompanied by AVN. If nonunion occurs, magnetic resonance imaging (MRI), which has largely supplanted scintigraphy in the evaluation of femoral head viability, should be used to evaluate vascular supply to the femoral head. Fixation of the femoral neck with titanium screws minimizes scatter of the MRI image that occurs with the use of stainless steel screws.
Options for treatment of nonunion include repeat internal fixation, bone or muscle-pedicle grafting, valgus osteotomy, and hip arthroplasty. In active patients, nonunion is treated with a valgus osteotomy and repeat fixation. In a series of 50 patients under 70 years of age who underwent valgus osteotomy for a nonunited femoral neck fracture, Marti and associates reported that 6 cases required reoperation because of technical complications, and 7 underwent later replacement (3 for persistent nonunion, 3 for severe osteonecrosis, and 3 for hardware breakage). At an average of 7 years’ follow-up of the remaining 43 fractures, AVN was evident in 22 but only 3 patients had symptoms severe enough that arthroplasty was required. In another series of 17 patients, union was achieved in all but 1 after osteotomy.
Five patients required an additional operation. Although the operation is difficult, based on their results, the authors of both studies recommended osteotomy in the younger, active patient with nonunion of the femoral neck. Muscle-pedicle grafting of femoral neck nonunions has been reported in a small number of cases,but this technique cannot be recommended on the basis of the available data. Since the majority of nonunions have drifted into some varus angulation, correction of the mechanical malalignment appears to be more essential than bone grafting. Muscle-pedicle grafting is unnecessary when a valgus osteotomy and fixation are performed to apply compression loads at the fracture site. Total hip replacement is the treatment of choice for nonunion in ambulatory, community based, elderly patients.
Avascular necrosis. Since the lateral epiphyseal artery, which supplies the majority of the femoral head circulation, runs in the superior capsule, it is at considerable risk after femoral neck fractures, particularly displaced fractures. As a result, most clinically relevant AVN follows displaced intracapsular fracture. Most studies report a 12% to 33% rate of osteonecrosis in displaced femoral neck fractures. Differences may be explained by the fracture type and by the authors’ method of reduction and fixation. Often, AVN does not involve the entire femoral head, and in many cases, collapse of the head does not occur.
The risk of developing AVN is directly proportional to the degree of displacement and the time to reduction. Operation within 6 hours of injury leads to improved union rates and a decreased incidence of femoral head collapse. Late-onset AVN is manifested by bone sclerosis, subchondral collapse, and eventual secondary degenerative changes of the hip. In the early stages of symptoms, when treatment may be beneficial, x-ray findings are normal, and at that point MRI provides the most sensitive and specific means of identification. However, MRI is unable to predict which intracapsular fractures will develop clinical AVN.
Several procedures can minimize the risk of developing AVN. Urgent reduction and fixation may be the most important. Several authors have shown that intracapsular fractures of the proximal femur result in markedly elevated intracapsular pressures secondary to hematoma formation.Using laser Doppler flowmetry, Swiontkowski and colleagues demonstrated significant diminution of femoral head blood flow with elevated intracapsular pressures in an animal model. Crawfurd and associates used ultrasonography to demonstrate capsular distension following both nondisplaced and displaced femoral neck fractures, and documented elevated intracapsular pressures associated with joint hemarthrosis.Some displaced fractures showed evidence of capsular disruption with extracapsular hematoma; this subgroup of hips had low intracapsular pressures consistent with decompression of the hip. Capsulotomy is recommended to relieve the intracapsular hematoma and restore blood flow.Stromqvist and colleagues showed that the intracapsular pressure is highest with the leg internally rotated and lowest in a position of mild flexion and external rotation. They also showed that following hip aspiration, intracapsular pressures fell to zero, and scintigraphic uptake increased in most hips, consistent with improved blood flow. Although the need for capsulotomy in femoral neck fracture remains controversial, the procedure is so simple to perform that it should be recommended.
Treatment of AVN, however, remains controversial. If the patient is asymptomatic, no further treatment is indicated. If collapse of the osteonecrotic fragment has occurred and the patient is symptomatic, total hip arthroplasty is indicated. The degree of radiographic involvement does not necessarily correlate with the severity of symptoms. In general, young, active patients will be more disabled by AVN than sedentary patients. Treatment options are based on age, activity level, and severity of symptoms. For the management of disabling symptoms in the community ambulator, total hip arthroplasty is recommended. As it remains unclear whether cemented implants offer advantages over uncemented implants, surgeons should select the technique and implant with which they are most familiar. In nursing-home patients, bipolar hemiarthroplasty should be performed. Core decompression, proximal femoral osteotomy, prosthetic replacement, and hip arthrodesis are rarely used.
Diagnosis
Often your doctor can determine that you have a hip fracture based on your symptoms and the abnormal position of your hip and leg. An X-ray usually will confirm that you have a fracture and show exactly where the fracture is on your bone.

If your X-ray doesn’t show a fracture but you still have hip pain, your doctor may order an MRI or bone scan to look for a small hairline fracture.
Most hip fractures occur in one of two locations on the long bone that extends from your pelvis to your knee (femur):
The femoral neck. This area is located in the upper portion of your femur, just below the ball part (femoral head) of the ball-and-socket joint.
The intertrochanteric region. This region is a little farther down from the actual hip joint, in the portion of your upper femur that juts outward.
A third type of hip fracture, called an atypical fracture, can occur in people who have been treated for a long period of time with medications that enhance bone density (bisphosphonates).
Treatment
Treatment for hip fracture usually involves a combination of surgery, rehabilitation and medication.
Surgery
The type of surgery you have generally depends on the location and severity of the fracture, whether the broken bones aren’t properly aligned (displaced fracture), and your age and underlying health conditions. The options include:
Internal repair using screws. Metal screws are inserted into the bone to hold it together while the fracture heals. Sometimes screws are attached to a metal plate that runs down the femur.
Total hip replacement. Your upper femur and the socket in your pelvic bone are replaced with prostheses. Increasingly, studies show total hip replacement to be more cost-effective and associated with better long-term outcomes in otherwise healthy adults who live independently.
Partial hip replacement. If the ends of the broken bone are displaced or damaged, your surgeon may remove the head and neck of the femur and install a metal replacement (prosthesis). Partial hip replacement may be recommended for adults who have other health conditions or cognitive impairment or who no longer live independently.
Your doctor may recommend partial or total hip replacement if the blood supply to the ball part of your hip joint was damaged during the fracture. That type of injury, which occurs most often in older people with femoral neck fractures, means the bone is less likely to heal properly.
Rehabilitation
Your care team will probably get you out of bed and moving on the first day after surgery. Physical therapy will initially focus on range-of-motion and strengthening exercises. Depending on the type of surgery you had and whether you have assistance at home, you may need to go from the hospital to an extended care facility.
In extended care and at home, you may work with an occupational therapist to learn techniques for independence in daily life, such as using the toilet, bathing, dressing and cooking. Your occupational therapist will determine if a walker or wheelchair may help you regain mobility and independence.
Medical treatment
Up to 10 percent of adults age 65 or older who have a hip fracture will have another hip fracture within two years. Bisphosphonates and other medications for osteoporosis may help reduce the risk of a second hip fracture. To avoid side effects that may make oral bisphosphonates difficult to tolerate, your doctor may recommend taking them via intravenous (IV) tubing.
Bisphosphonates generally aren’t recommended for people with kidney problems. Rarely, long-term bisphosphonate therapy might cause pain and swelling in the jaw, vision problems, or an atypical hip fracture.
Physiotherapy treatment:
I. Areas to evaluate for femoral neck fracture physiotherapy
A. Postoperative evaluation
- Two to three days postoperative
a. Evaluate gross muscle strength and range of motion of other extremities.
b. Observe gross muscle strength of involved extremity by strength of isometric muscle contractions.
c. Assess sensation of involved extremity.
d. Assess range of motion of involved hip within limits of pain.
- Three to five days postoperative
a. Evaluate gait pattern with assistive device.
b. Evaluate functional ability with regard to transfers and bed mobility.
c. Continue to evaluate gross strength of involved extremity.
B. Outpatient evaluation
- Complete specific muscle tests on all groups.
- Test range of motion of hip, knee, and ankle.
- Analyze gait.
- Evaluate functional ability.
- Complete specific tests, including Functional Ambulation Profile and Get Up & Go Test.
II. Precautions during evaluation
A. Weight-bearing status must be determined by physician.
B. Assess cardiac status prior to initiation of evaluation.
Treatment/Goals
Mobilisation after fracture: Femoral neck fracture Physiotherapy
Patients with cemented joint replacements can weight bear as tolerated (WBAT) unless the operative procedure involved a soft-tissue repair or internal fixation of bone.
Patients with cementless, or ingrowth , joint replacements are put on partial weight bearing (PWB) or toe-touch weight bearing (TTWB) for 6 weeks to allow maximum bony ingrowth to take place.
I. Frequency
A. Inpatients should be seen daily, twice if possible.
B. Outpatients are followed as necessary.
II. Treatment techniques and goals
A. Two to three days postoperative
- Instruct patient in deep breathing and cough. Goal: Prevent postoperative pneumonia and atelectasis.
- Initiate isometrics and ankle pumps with involved extremity. Goal: Prepare patient for active exercise program.
- Initiate bedside sitting once physician has cleared patient for this activity. Goal: Prepare patient to begin transfer and progressive gait training processes.
B. Three to five days postoperative
Gait train patient, observing weight-bearing precautions. Progress to walker or crutches. Goal: Establish independent gait with assistive device, using proper gait pattern on all surfaces and stairs.
Initiate training in activities of daily living, including bed mobility and transfers to and from bed and toilet. Goal: Achieve independence with all transfers.
Initiate active range of motion/strengthening program. Individualize exercise program according to each patient’s needs, but generally include the following. Goals: Increase strength of involved extremity; increase independence with exercise program.
a. Supine: hip abduction and adduction, gluteal sets, quadriceps sets, straight leg raise, hip and knee flexion, short arc quadriceps, internal and external rotation.
b. Sitting: Long arc quadriceps, hip flexion, ankle pumps.
III. Equipments
A. Bilateral support assistive devices (crutches or walker).
B. Other adaptive equipment as necessary for independence.
IV. General considerations
A. Evaluate patient’s home situation to determine need for additional equipment, home health physical therapy services, or other support.
B. Request physician consult for necessary equipment or other needs.
Discharge
I. Evaluation. Make final assessment of patient’s functional level, gait, range of motion, and strength.
II. Follow-up plan/referral
A. Continue outpatient physical therapy program as indicated.
B. Initiate home health physical therapy services when indicated.
III. Home program
A. Educate patient and family on exercise program.
B. Provide written home exercise program.
Femoral Neck Fracture Physiotherapy Management in Detail
Femoral neck fracture Physiotherapy Management after Surgery
During the 1st week: Femoral neck fracture Physiotherapy Management
The wound is inspected for evidence of infection and the drains are removed after 24 hours. Pulmonary embolism and hypovolaemia are a distinct possibility and a careful watch is kept to prevent bedsores from developing, the patient is frequently turned in the bed. Derotation bar helps prevent external rotation of the affected limb. Patients treated with hemiarthroplasty should avoid keeping the hip in adduction or internal rotation to prevent redislocation.
a. Movements: A full range active movements of the ankle, gentle active movements of flexion and extension of the hip and knee (once the pain subsides) is permitted. Caution: No passive range of motion at this stage.
b. Exercises: After the pain subsides, isometric gluteal and quadriceps exercises are begun. Isotonic exercises are prescribed for the ankle as it helps to strengthen the gastro-soleus muscle and reduces the chances of thrombophlebitis and deep vein thrombosis.
c. Weight-bearing: By the end of first week, weight bearing with the help of a crutch or walker using a 3-point gait may be permitted. However, it is deferred in unstable fractures. For patients with endoprosthesis, weight bearing as tolerated is permitted.
d. Activities of daily living: Certain modifications are brought about in the activities of daily living. Use of raised toilet seat and chair, wearing the trousers from the affected limb first and removing it from the unaffected limb, rolling on to the unaffected side before getting up from the bed are some of the recommended modifications in daily living.
During 2-4 weeks: Femoral neck fracture Physiotherapy Management
a. Movements: Active and active-assistive movements of the hip, knee and ankle can now be started. However, no passive movements are still recommended.
b. Exercises: Ankle isotonic exercises are continued. Isometric exercises for the hip and knee are prescribed.
c. Weight-bearing: This has to be done on the following lines:
- First the patient is advised prone lying.
- Next as a preclude to weight bearing, four point kneeling is advised.
- Then patient is advised to bear weight on the knees.
- Next, knee walking is encouraged.
- Patient may now be allowed to bear the weight on the affected extremity either partially or fully depending on the stability of the fracture. A 3-point gait using crutches or walker is advised.
d. Activities of daily living: Modifications in activities of daily living are the same as mentioned earlier.
during 4-8 weeks: Femoral neck fracture Physiotherapy Management
The treatment regimen is more or less the same as discussed above. The patient can now flex the hip upto 90 degree, by the self-assisted “heel drag”, (i.e. dragging the heel upto the buttocks with the help of the normal leg). The patient can now be encouraged to sit with the legs hanging over the edge of the bed and supporting and lifting the affected limb with the unaffected leg. Assisted and self-resistive exercises for the hip and knee muscles can be carried out.
After 8 weeks: Femoral neck fracture Physiotherapy Management
Passive range of movements by the physiotherapist or by continuous passive motion apparatus is begun to the hip and knee. Isotonic and isokinetic exercises to the hip and knee are initiated alongwith progressive resistive exercises. Weight-bearing with the affected extremity with the help of crutches or walker using a four point gait can be initiated as the patient can bear more weight now. Activities of daily living can be allowed normally with the help of assistive devices.
However, excessive adduction and internal rotation should be avoided in patients treated with endoprosthesis.
By 12-16 weeks: Femoral neck fracture Physiotherapy treatment
Full weight-bearing is allowed. Full active and passive range of motion exercises are permitted to the hip and knee joints. Isometrics, isotonic and progressive resistive exercises are continued to the hip, knee and ankle joints. Patient can now carry out all the activities of daily living independently.
The physiotherapy regimen is more or less the same for patients treated with hemiarthroplasty (the emphasis is on to prevent adduction and internal rotation to prevent redislocation), McMurray’s osteotomy, Meyer’s muscle pedicle graft, etc.


One Comment