
Brachial Plexus Injury and Treatment
Table of Contents
Overview:
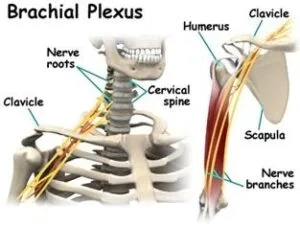
The brachial plexus is the leading network of nerves that gives signals from the spinal cord to the shoulder, arm, and hand. It provides movement and sensation in the arm and hand. The brachial plexus starts at the neck and cross the upper chest to the axilla. Brachial plexus injury occurs when the arm is forcefully pulled or stretched.
Brachial plexus injury occurs when the nerves are overstretched, compressed, or torn from the spinal cord. Most commonly this injury happens in automobile or motorcycle accidents. In A traumatic brachial plexus injury the sudden damage to these nerves, and results in weakness, loss of feeling, or loss of movement in the shoulder, arm, or hand.
Minor brachial plexus injuries are known as stingers, and they are commonly seen in contact sports, like football. Sometimes sustained brachial plexus injuries are seen in babies during birth. Other conditions, like inflammation or tumors, may affect the brachial plexus. Mild brachial plexus injuries may heal without surgical treatment. More severe injuries result in the arm being paralyzed and may require surgery to restore the arm or hand function.
Traumatic incidences of brachial plexus injuries are often leading to severe social and financial hardships and more affecting the quality of life.
What is brachial plexus?
The brachial plexus meaning is BRAY-key-el PLEK-sis. It is present on each side of the body.
The brachial plexus is a bundle of nerves that is situated from nerve roots in the cervical (neck) and upper trunk sections of the spinal cord (C5-T1) and it creates a network that connects to the nerves in the arm. These nerves control the movement and provide the sensation to the wrists, hands, and arms.
This nerve complex has four cervical nerve roots (C5 to C8) and the first thoracic nerve root (T1). These nerve roots together form three trunks. C5-C6 make the upper trunk, C7 as the middle trunk and C8-T1 make the lower trunk.
Each trunk has a different division. Half the divisions of the trunk supply flexor muscles and the others supply the extensor muscles.
Anatomy of Brachial plexus:
The brachial plexus nerve roots are divided into a few different sections: trunks, divisions, cords, and branches. These sections are not functionally different from each other, but help to know the complex anatomy of the brachial plexus.
Root
The anterior primary rami of spinal nerves C5, C6, C7, C8, and T1 also contribute to the anterior primary rami of C4 and T2. The arising of the plexus may shift one segment upward or either downward and resulting in a pre-fixed plexus or post-fixed plexus respectively.
In a prefixed plexus, the contribution of C4 is large, and in that T2 is often absent. In a post-fixed plexus, the contribution of T1 is large, T2 is always present, C4 is absent and C5 is decreased in size. The roots are fused and form the trunks are following:
Trunk:
- The upper trunk is formed by C5 & C6
- The middle trunk is formed by C7
- The lower trunk is formed by C8 & T1
Trunk Divisions:
Each trunk divides into ventral and dorsal divisions. These divisions form the cords.
Cords:
- The Posterior Cord is formed by the three posterior divisions of the trunks (C5-C8, T1).
- The Lateral Cord is formed by anterior divisions of the upper and middle trunks (C5-C7).
- The Medial Cord is continue as the anterior division of the lower trunk (C8, T1).
Cord continues to as a nerve at a different level. Five major nerve branches are following:
- Musculocutaneous nerve: It starts from C5-C7 nerve roots and this nerve gives the flexion movement of the shoulder and elbow.
- Axillary nerve: Starts from nerve roots C5 and C6; it helps the shoulder rotation and can’t do the arm lift up.
- Median nerve: Starts from nerve roots C6-T1.
- Radial nerve: It starts from the nerve roots of C5-T1 and controls various muscles in the upper arm, elbow, forearm, and hand.
- Ulnar nerve: It starts from C8-T1, it allows for fine motor control of the fingers.
Every nerve has a specific function, like muscle movements or carrying sensory information from the hand to the brain.
What is brachial plexus injury?
The brachial plexus is a wide network of upper extremity nerves. It controls the movement and sensation in the arm and hand.
It starts from the spinal cord roots and extends to the armpit. A brachial plexus injury may cause pain, weakness, loss of sensation, or loss of movement in the upper extremity.
This Injury happens when the arm is forced fully pulled, stressed, ed, or stretched, and during the birth baby’s head and neck are forcibly pulled from the shoulder. Brachial plexus injury in babies is known as Neonatal Brachial plexus injury. The nerves are also damaged by cancer or radiation treatment and the overactive immune system of the body.
In the brachial plexus injuries cut all parts of the communication between the spinal cord and the upper extremity. Due to that person can’t move or feel parts of the arm or hand. The severity of a brachial plexus injury is different. In some cases, function and feeling return to normal but Others may have lifelong disabilities.
What are the causes of brachial plexus injury?
Most commonly brachial plexus injuries occur when the arm is forcefully pulled or stretched. Other causes of injury are falling from a height, motor vehicle accidents, and knife and gunshot injuries.
It is not exactly known how many brachial plexus injuries occur every year, but the number of these injuries is growing worldwide. Upper nerves are damaged when the shoulder is forced down, the neck stretches up away from the injured shoulder. The lower nerves are to be injured when the arm is forcefully stressed above the head.
These injuries can occur in many different causes are following:
Contact sports (Athletic injuries): Football players experience burners or stingers, which can occur when the plexus nerves get stretched above their limit during playing.
Difficult births: Sometimes newborn babies have sustained brachial plexus injuries. These may happen when high birth weight baby, breech presentation, and prolonged labor. Mostly the upper nerves are injured in infants.
Blunt Trauma: many different ways including motor vehicle accidents, motorcycle accidents, and falls from height.
Gunshot wounds: In a gunshot a bullet tears through the nerves.
Tumors and cancer treatments: If the radiation treatment given to the chest or neck area may cause grow the tumors to grow in the brachial plexus, or the pressure is generated on the brachial plexus and spread to the nerves so that the brachial plexus is damaged.
Medical trauma: Brachial plexus injury happen when a nerve is cut during any surgical procedure, the nerve is damaged by any anesthetic injection, and the body is positioned during surgery.
Mechanism of injury:
Brachial plexus injury can occur in many different ways. These include contact sports, road traffic accidents, motor vehicle accidents,s or during birth. it is divided into 2 types.
- Traumatic: motor vehicle accident, contact sports
- Nontraumatic: obstetric palsy and Parsonage-Turner Syndrome
The network of nerves is easily damaged by stretching, pressure, or cutting.
Stretching can happen when the head and neck are forced fully pulled from the shoulder, another one is a fall from a motorcycle. In that, the nerves can be stretched, or torn out of their roots in the neck.
Pressure is generated from crushing of the brachial plexus between the collarbone and first rib or swelling in this area from injured muscles or other structures. The traction and heavy object occur the brachial plexus injury.
Traction: It is also known as stretch injury. It is one of the mechanisms that cause brachial plexus injury. The brachial plexus nerves are damaged due to the forced full pull of the shoulder and neck so that tension is generated on the nerves. Mainly the two types of traction are downward traction and upward traction.
- In downward traction: There is tension on the neck and shoulder to become broader. This tension is generated on the upper roots and trunk of the brachial plexus’s nerve.
- In Upward traction: There is broadening between the arm and chest angel when the arm and shoulder are forced in an upward direction. so that the nerves of C8 and T1 are torn away.
Heavy Impact: It is the second most common mechanism of causing injury to the brachial plexus. The area of impact also affects the severity of the injury and depends on which nerve is injured. Other ones that affect the injury to the brachial plexus are shoulder dislocation, clavicle fractures, hyperextension of the arm, and sometimes delivery at birth.
Symptoms of Brachial plexus injury:
Symptoms depend upon the type and location of the brachial plexus injury. The symptoms of brachial plexus injury following:
- Weakness or numbness in the upper extremity.
- Loss of sensation.
- paralysis(Loss of movement) in your arm and hand.
- Pain is neuropathic in nature; it is increasing over time and becomes chronic.
- Injury is near the spinal cord patient has felt like burning sensation, which is called paresthesias or dysesthesias.
- An arm that hangs limply.
- Injury to the higher nerve root of the spinal cord, in the neck, affects the shoulder. If an injury is in the lower brachial plexus nerve, the arm, wrist, and hand are affected.
- Inability to control or move the shoulder, arm, wrist, or hand.
- Burning or severe and sudden pain in the shoulder or arm.
Symptoms of a brachial plexus injury in infants are the following:
- Loss of movement in your newborn’s upper or lower arm or hand.
- Absent Moro reflex (startle response) on the affected side.
- They hold their arm against their body with their arm extended (straight) at their elbow.
- Reduced grip strength on the affected side.
What are the types of Brachial Plexus injury?
Brachial plexus injuries is depending on the type of injury and the amount of force which are involved. The common types of brachial plexus injuries are the following:
Neuropraxia (Stretch) :
It happens when a brachial plexus nerve mildly stretches, which damages the covering of the nerve so that the conduction of the nerve is altered. Mainly compression and traction are these 2 ways affecting nerve injury.
In Compression neuropraxia, the nerve roots are compressed by the rotation of the head. it is generally seen in older people.
In Traction neuropraxia, the nerve roots are pulled downwardly. It is generally seen in adolescents and young adults. In the neuropraxia type of injury physical therapy helps to return the normal function.
Brachial plexus Rupture:
This happens when a forceful stretch of a brachial plexus nerve causes a tear partially or completely. It is a serious type compared to neuropraxia. It can cause weakness and pain in the upper extremity. This type of injury can often be repaired with surgery.
Brachial plexus Avulsion:
It is the most severe type of brachial plexus injury. In that, the nerve is completely torn or separated from the spinal cord. It is caused by any type of accident. It can lead to permanent weakness ad paralysis so this injury requires surgery to regain function.
Brachial Plexus Neuroma:
Sometimes when nerve tissue is cut during surgery, scar tissue can form as the nerve repair itself. This scar tissue is called a neuroma, and it may result in pain in the brachial plexus nerve. In the brachial plexus, neuroma treatment does the surgical removal of the scarred nerve tissue. The surgeon then either caps to the nerve or attaches it to another nerve to prevent another neuroma from forming.
Brachial Neuritis:
It is Also known as Parsonage-Turner syndrome, brachial neuritis is rarely seen. It is a progressive disorder of the brachial plexus nerve. This syndrome causes severe shoulder and upper arm pain and progresses to the weakness of muscles and decreases sensation. This syndrome affects the shoulder, arm, legs, and diaphragm.
Classification of injuries:
The different classifications of brachial plexus injury are as follows:
Leffert classification of brachial plexus injury (based on causes and level of injury):
Open (from stabbing)
Closed (from a motorcycle accident)
Supraclavicular
Radiation
Obstetric
Erb’s palsy (upper root) – waiter’s tip hand;
Klumpke (lower root)
Millesi classification of brachial plexus injury:
supraganglionic/preganglionic
infraganglionic/postganglionic
trunk
cord.
Classification of the anatomical location of injury:
Upper plexus injury (Erb’s palsy in the OBPI cases) involves C5-C6+/-C7roots
Lower plexus injury(Klumpke’s palsy) involves C8-T1 roots (and sometimes also C7)
Total plexus lesions involve all nerve roots C5-T1.
Injuries related to the brachial plexus:
Injuries to roots, trunks, and cords of the brachial plexus resulting defects which are the following:
Erb’s Paralysis:
The area of the upper trunk of the brachial plexus is called Erb’s point. Six nerves meet here. Injury to the upper trunk is called Erb’s Paralysis. mainly C5 and sometimes C6 nerve roots involved.
It causes the pulled the head from the shoulder like during birth injury, falls on the shoulder, and during anesthesia. In this paralysis, the bicep, deltoid, brachialis and brachioradialis, supinators, supraspinatus, and infraspinatus muscles are paralyzed. So that the deformity is produced in the arm and forearm. That deformity is known as “Policeman’s tip hand” or “Porter’s tip hand”.
Disability:
Abduction and lateral rotation movement of the shoulder.
Flexion and supination of the forearm.
Biceps and supinator jerks are diminished.
Sensations are lost over a small area of the lower part of the deltoid.
Klumpke’s Paralysis:
In this type of Injury, the Lower trunk of the brachial plexus is affected. It causes when the arm in force fully abducted like fall from a height during clutching a tree branch or sometimes in a birth injury. Mainly T1 or C8 nerve roots are involved in this type of paralysis so that the intrinsic muscles of the hand and ulnar flexors muscles of the wrist and fingers are paralyzed.
In the klumpkes paralysis, the claw hand deformity is present.
Disability:
Horner’s syndrome: ptosis, miosis, anhydrosis, and enophthalmos symptoms present due to the injury of sympathetic fibers of the head and neck that are torn to the spinal cord.
Vasomotor changes: Sensory loss in the affected skin area.
Tropic changes: chronic stage of paralysis leads to dry and scaly skin. The nails brake easily with atrophy of the pulp of fingers.
Injury to lateral cord:
When the dislocation of the humerus is occur due to any injury the lateral cord of the brachial plexus is affected. in this injury, the musculocutaneous nerve and lateral root of the median nerve are affected. so that the biceps muscle and coracobrachialis muscles are paralyzed. In this injury flexion movement of the forearm and wrist are affected. Sensory loss is present on the radial side of the forearm.
Injury to medial cord:
Its cause is Subcoracoid dislocation of the humerus. the ulnar and medial root of the median nerve is injured. Muscles that are supplied by the ulnar nerve are paralyzed and hand muscles that are paralyzed are supplied by the median nerve. Claw hand deformity is present in this injury.
Risk factors of the Brachial plexus injury:
Playing in contact sports, especially football players and wrestling persons, high-speed motor-vehicle driving increases the risk of brachial plexus injury.
Breech delivery, obese mother and newborn child are in big size, shoulder dystocia is risk factors affected in the neonatal brachial plexus injury.
When to see a doctor?
Brachial plexus injuries can occur permanent weakness or disability. if symptoms are minor, in the early stage patient goes and meets the doctor. if a patient has felt any abnormality or pain in the body consult the doctor for an early period time.
Diagnosis of the Brachial plexus injury:
Physical Examination:
If the person has a brachial plexus injury, the doctor will take a comprehensive examination to diagnose the injury and check if any other injuries are present or not, which happen due to brachial plexus injuries. The doctor checks all the nerve groups and identifies the specific location and severity of the injury.
If the newborn baby comes so doctor first takes the whole history for them and checks all reflexes and movements of the affected side.
Patients with brachial plexus injuries must be diagnosed and treated at an early time within 6 to 7 months after injury. It depends on the type of injury and its location. Smaller eye pupils, drooping of the eyelid, and lack of sweating on the face (Horner’s syndrome) are signs that the injury occurs to the spinal cord.
Tinel’s sign is present it suggests an injury further from the spinal cord.
The doctor will also check the patient’s arm and shoulder for stability and range of motion. The doctor checks any other imaging tests to confirm the diagnosis and check for further injuries.
Imaging Tests:
X-rays: X-rays give clear pictures of bony structures. Get X-rays of the neck, chest, shoulder, and arm to rule out associated bone fractures. these parts injuries occur in the traumatic injuries.
Nerve conduction studies: It measures the nerve signals traveling in the muscles of your arm and hand.
Computed tomographic (CT) scan: It is the most confirmatory test for detecting spinal nerve injuries. Contrast dye is inserted around the spinal cord in the neck to show a more clear picture of the injury on the CT image. this test is performed at least 3 to 4 weeks after the injury. Some doctors may also use a magnetic resonance imaging (MRI) scan instead of a CT scan.
Electrodiagnostic studies: These tests measure nerve conduction and muscle signals. They are important diagnosis studies because they can confirm the diagnosis of brachial plexus injury, locate the nerve injury, and its severity, and assess the rate of nerve recovery. An electrodiagnostic examination is done 3 to 4 weeks after the injury. If any nerve becomes degenerate that may detect in these studies. These are repeated 2 to 3 months after the one study and then repeatedly over time to assess whether the nerves are recovering or not.
If the infant has a brachial plexus injury, the doctor may suggest an X-ray of the collarbone to see if it’s fractured.
Neonatal brachial plexus injuries can imitate a condition called pseudoparalysis. In that infant has a fracture and can’t move their arm because of pain, not because of the nerve damage.
Treatment of Brachial plexus injury:
The brachial plexus injuries are typically caused by traumatic and other forceful events. Many people have some additional injuries along with the brachial plexus injury that as the following:
- Artery or vein injuries.
- Shoulder, arm, spine, or rib fractures.
- A collapsed lung.
- Spinal cord injury.
- Traumatic brain injury.
Because of this, firstly doctors treat these life-threatening injuries before they treat the brachial plexus injury.
A brachial plexus injury is treated by a whole medical professionals team that may be the following:
- Neurologist.
- Neurosurgeon.
- Hand surgeon.
- Physical therapist.
- Occupational therapist.
- Primary healthcare provider.
The two main types of treatment for brachial plexus injuries: An Nonsurgical and Surgical treatment.
Nonsurgical Treatment:
Mild brachial plexus injuries will recover spontaneously without surgery over a period of weeks to months, Nerve injuries that heal on their own tend to have better functional results. If a doctor believes that the injury has a good recovery without surgery, so the doctor simply monitors the recovery of an injury.
The doctor recommended physical therapy as the injury heals to prevent joint and muscle stiffness and advised them to patient avoid strenuous activities.
Cortico steroids and creams help to decrease the pain during healing.
Surgical treatment:
Doctors suggested surgical treatment for brachial plexus injuries when the nerves don’t heal on their own or can’t chance recover their function. Surgeons use many different techniques to treat nerve injuries, depending on the type and severity of the injury and the total time period of injury that has passed.
Types of surgical procedures include:
Nerve repair: In this procedure, the surgeon attaches the two torn edges of an injured nerve. Surgeons do this type of procedure when the injury happens to any sharp object.
Nerve graft: In this procedure, the surgeon takes a nerve from another part of your body and attaches it between the two ends of an affected nerve.
Nerve transfer: Surgeons do this procedure when there are no functions of nerve in your neck to which nerve grafts can be connected. In this procedure, the surgeon cuts and reconnects a healthy nerve to the injured nerve to provide a signal to a paralyzed or affected muscle.
Treatment for the neonatal brachial plexus injury:
If the infant has a mild brachial plexus injury, the doctor will recommend gently massaging their arm and range-of-motion exercises for treatment.
If the condition is severe or it doesn’t improve the condition within the 3 to 9 months of age so the neurosurgeon advised the surgery.
Physiotherapy Treatment for Brachial plexus Injury:
Physiotherapy treatment for brachial plexus injury is different and it depends on the type and severity of the injury. In mild cases physiotherapy and rehabilitation will assist the recovery of nerve, in more severe cases surgery and bracing may be required.
physiotherapy goal is to return or achieve the previous level of function and prevent another disability.
Physiotherapy treatment aims:
- Increase in strength, flexibility, stamina, and coordination.
- Maintaining ROM via passive movements, exercise therapy, splinting, and positioning of the affected muscles.
- Functional training and orthosis devices use if needed.
- Decrease the pain.
- Managing chronic edema.
Physiotherapy treatment following:
- Decrease the pain by giving the TENS.
- Range of motion of the affected part
- Strengthening exercise of the affected upper extremity.
- Neuromuscular electrical stimulation for the nerve becomes regenerated.
- Kinesio Taping
- Joint mobilization of the affected limb.
- Aquatic therapy.
- Use of orthoses or splint
- Constraint-induced movement therapy.
- virtual reality.
- Exercises like shoulder extension, flexion, elevation, depression, abduction, and adduction encourage the healing of injured nerves in the damaged sites as well as improve muscle function.
- Stretching is done to improve or maintain range of motion. It also facilitates nerve functions.
- Balance exercises according to the patient BBS SCORE.
- Advised with assistive devices such as splints, braces, and compression sleeves.
Physiotherapy Treatment after the surgery for Brachial Plexus injury:
Surgery is advised in severe brachial plexus injuries. Surgery aims to regain function through a different surgical procedure.
Physiotherapists are given treatment in the rehabilitative phase after surgery to restore the function via strength, coordination exercises, flexibility, ROM, power, and the use of splinting if needed. The patient needs to be aware that the rehabilitation phase will take years not weeks.
Complications of the Brachial plexus injury:
Many brachial plexus injuries in children and adults have healed in a short duration time. But some injuries can occur the temporary or permanent problems, like;
- Stiff joints: In the paralysis condition the arm and hand become stiff. so that it is difficult to move. so, the doctor recommended physical therapy during the recovery.
- Pain: Pain is generated due to nerve damage or chronic condition.
- Numbness: The patient has a loss of sensation and feels like a burning sensation.
- Muscle atrophy: Nerves regeneration becomes slow and can take several years for healing after injury. that time those muscles are not used they become atrophied.
- Permanent disability: The recovery from a serious brachial plexus injury depends on different factors like the person’s age and the type, location, and severity of the injury. Even after the surgery, some have experienced permanent muscle weakness or paralysis.
- Heart attack.
- Blood clots.
All surgeries have risks of some possible complications, following:
- Any anesthesia.
- Infection.
- Excessive blood loss.
Prevention for the Brachial plexus injury:
For the patient: The patient can’t use the hand or arm in daily activity and joint range of motion are limited. Physiotherapy can help prevent joint stiffness. if the person is an athlete therapist advised him to wear specific padding to protect the injured area during sports.
For the child: If a child with a brachial plexus palsy, daily exercise is a must for the child’s joints and functioning muscles every day, Exercise starts from starting weeks of injury. This helps to prevent the joints from becoming permanently stiff and keeps your child’s working muscles strong and healthy.
Prognosis of the Brachial plexus injury:
The prognosis of brachial plexus injuries depends on some different factors, following:
- The type and severity of nerve injury (avulsion, rupture, or stretching).
- Depends on Which nerve(s) were damaged.
- If you had some previous injuries.
- When patients take treatment after the injury.
For avulsion and rupture injuries, generally, no functional recovery unless the patient is done with the surgical procedure of nerves in an early period of time. People who have stretch injuries (neuropraxia). It was recovered without surgery with a 90% to 100% return of nerve functions.





3 Comments