Thumb Collateral Ligament Injury
Table of Contents
Introduction
The thumb collateral ligament is a band of tissue that connects the thumb bone to the hand bone on the side of the thumb. A thumb collateral ligament injury can occur when the ligament is stretched, partially torn, or completely torn.
Symptoms of a thumb collateral ligament injury may include pain, swelling, bruising, weakness, and instability in the thumb. If you suspect you have a thumb collateral ligament injury, it is important to seek medical attention for an accurate diagnosis and appropriate treatment.
Treatment for a thumb collateral ligament injury may include rest, ice, compression, and elevation of the affected thumb to reduce swelling and pain. A doctor may also recommend a thumb brace or splint to support the thumb and allow it to heal. In some cases, surgery may be necessary to repair a completely torn ligament.
Rehabilitation exercises may be recommended to help restore strength, flexibility, and range of motion in the thumb. It is important to follow your doctor’s instructions and attend all recommended appointments to ensure proper healing and recovery from a thumb collateral ligament injury.
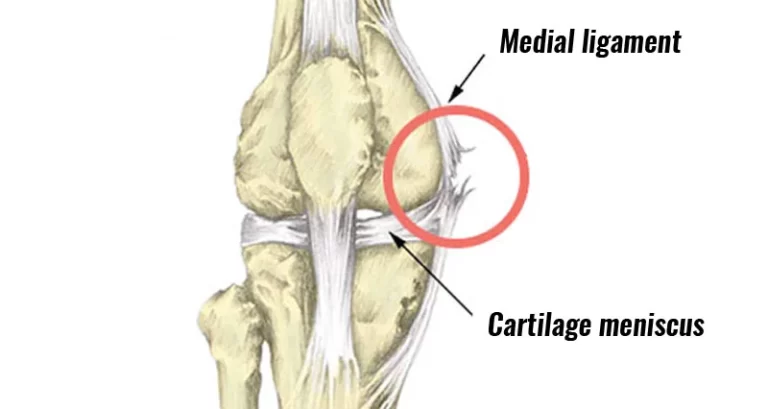
Two main ligaments provide stability to the MCP joint of the thumb the ulnar collateral ligament (UCL) and the radial collateral ligament (RCL)
Ligaments are powerful, fibrous tissues that normally join bones to bones. The ligaments in the thumb support maintaining the bones in a suitable place while allowing for motion in the joints.
Sprains happen when the ligament is prolonged and stretched above its limitation, which can also result in little, incomplete tears in the fibers that drive up the ligament. The ligament, yet, stays undamaged. These insufficient tears are commonly called partial-thickness tears. Ligaments can even be ripped completely— either in the center of the ligament or at the end(s) of the ligament, where it can pull off the bone.
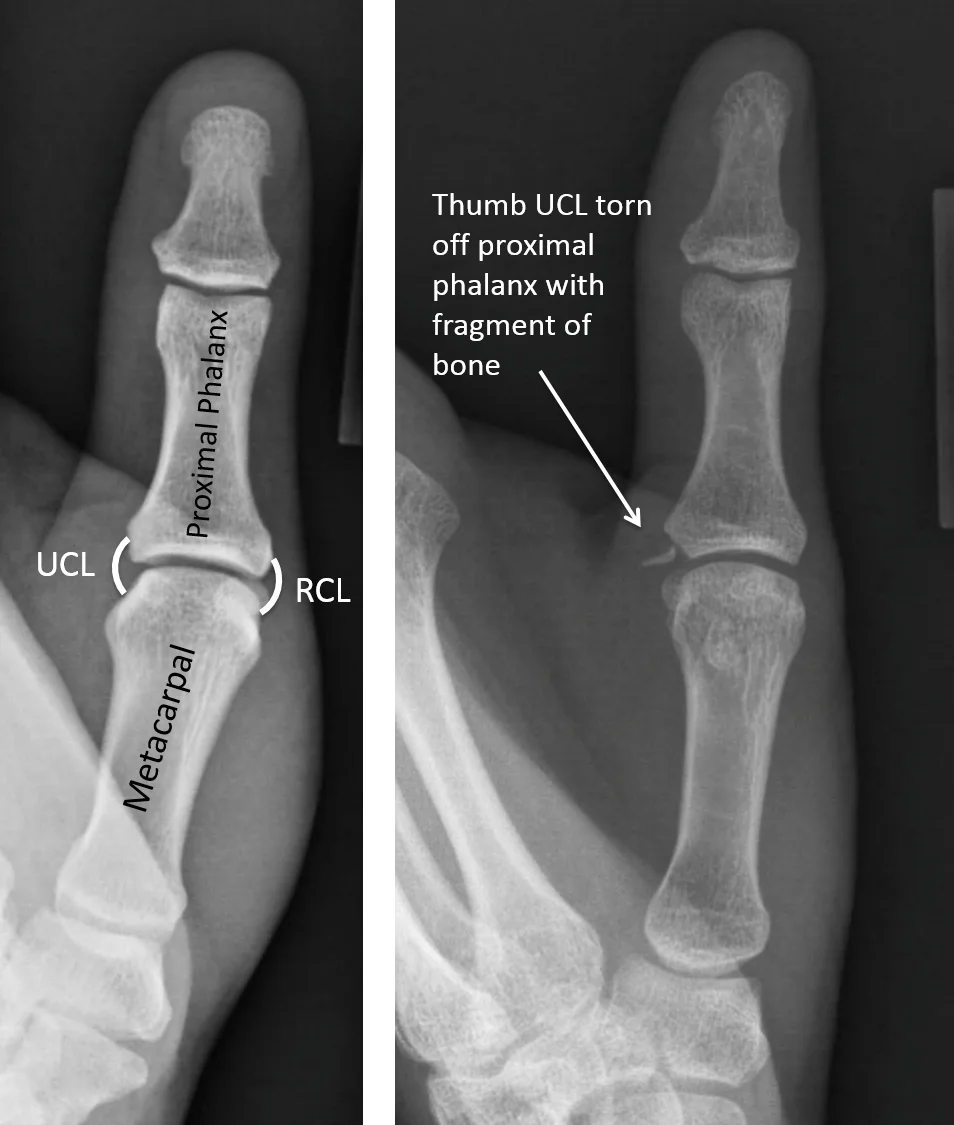
These are significant damages that need medical or surgical care. If the ligament completely rips out from its insertion, it may take a small fragment of the bone with it. this is named an avulsion fracture.
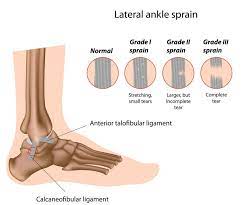
Grades of Thumb Sprains
Sprains are graded depending on the extent of injury to the ligament:
- Grade 1 sprain (mild). The ligament was not torn only stretched.
- Grade 2 sprain (moderate). The ligament is partially torn. This kind of damage may affect some loss of function.
- Grade 3 sprain (severe). The ligament is fully torn in the middle or is pulled off its insertions to the bone.
These are significant damages that need medical or surgical care. If the ligament is pulled out from its insertion, it may take a small fragment of the bone with it. this is named an avulsion fracture.
Clinical Anatomy
The thumb MCP is very exact in anatomical formation to those of the digits of the hand but primarily functions as a hinge or ginglymus joint. The articular morphology seen in this joint causes the most various movement of all joints, with a range of motion of 6 to 86 degrees in the sagittal plane which is flexion-extension movement
- Flexor pollicis brevis (FBP)
- Abductor pollicis brevis (APB) muscles insert partially on the sesamoids and provide proper stability in front of hyperextension forces.
- The ligamentous anatomy is similar to that found in the digits of MCP joints, with extrinsic tendons supplying extra support
Mechanism of Injury
The Metacarpophalangeal (MCP) connects the thumb and is supported by two primary ligaments. The ulnar collateral ligament (UCL) and other the Radial collateral ligament (RCL). Among both ligaments, UCL is more prone to damage, primarily from forced radial deviation (abduction) of the thumb, while the RCL is infrequently injured. Nevertheless, in extreme kinds of damage, both ligaments may be damaged.
Symptoms of Thumb Collateral Ligament Injury
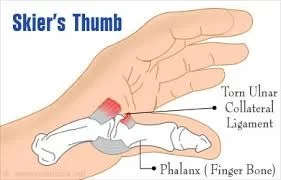
Thumb ligament traumas commonly happen from a forced radial deviation (abduction) of the thumb during a high-velocity action. Skiers and those individuals who have an interest in playing ball-handling games, for example, baseball, football, and basketball, have more venerable to occur such types of trauma Skiers can damage the thumb ligament in accidents concerning the ski poles or from a drop.
Ball-handling players frequently support thumb damage when the ball strongly abducts the digit, causing a UCL tear.
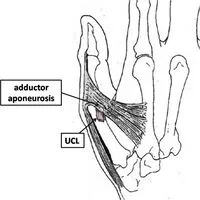
Stener lesions: when the thumb is in a hyperextended position at the time the ball hits, the RCL can be torn instead.(Capsular damages or sterner lesions. A Stener lesion is an X-ray finding suggesting a total rupture of the UCL with the adductor aponeurosis interposed between the avulsed ligament(distally) and it’s the base of the proximal phalanx.
Relying on the harshness of the sprain, you can or can not encounter pain during the duration of the injury.
You can have bruising, tenderness, and swelling near the base of your thumb, near the palm.
If the ulnar collateral ligament is fully torn, the end of the damaged ligament may result in a lump or swelling on the interior of the thumb. The thumb joint can also sense loose or inconsistent. You may have tribulation on grasping objects between your thumb and index digits.
Complications of Thumb Collateral Ligament Injury
- Changed sensation feeling near the incision site and along the thumb
- Joint stiffness
- Persistent instability
- Arthritis of the thumb joint
Differential Diagnosis
- First metacarpal or proximal phalanx fractures
- First CMC joint arthritis
- Volar plate injury
Diagnostic Procedures
Taking the history of the patient, involving mechanism, the position of the finger when the injury happen, the presence of deformity, prior therapy acquired, and personal feeling of stability of the injured thumb.
- Neurovascular assessment should specify motor impairment, perfusion, and sensation.
- Weakness with pinch grip is commonly present in ligament damage.
- Inspect the base of the thumb for ligamentous laxity and correspond it to the intact other hands:
- Assess the thumb with 20–30 degrees of flexion.
- Carefully abduct the thumb passively and correspond the angle of the tangent to the uninjured thumb.
- X-ray must be brought to evaluate for the existence of a Stener’s lesion or a fractured segment.
- Additional examination of the joint must be performed utilizing a digital block may be required to conduct a complete assessment due to the pain and swelling in acute cases.
Treatment of Thumb Collateral Ligament Injury
Conservative management
Mild thumb sprains will normally recover with home therapy that possesses the RICE program:
- Rest. Do not utilize your hand for at least 2 days from the time of injury.
- Ice. Use ice instantly after the trauma to reduce the swelling. Utilize the cryotherapy technique for twenty minutes at a time, various times a day. Do not use ice instantly on the skin.
- Compression. Wear an elastic compression bandage to decrease the swelling. Do not make the bandage too close-knit, as this can block the blood circulation to the thumb.
- Elevation. As frequently as potential, rest with your hand raised more elevated than your heart level.
- Further, nonsteroidal anti-inflammatory drugs (NSAIDs), for example, aspirin or ibuprofen, can assist to relieve pain and decreasing swelling. If, yet, pain and swelling persist for more than two days, see a doctor.
A thumb spica splint or cast immobilization is suggested for four weeks for a partial rupture, or up to 6 weeks if related to an avulsion fracture exists.
For acute injury:
- Rest, elevation, ice, compression
- Immobilization in a thumb or cast immobilization
- Analgesics Drugs
- Orthopedic follow-up
For chronic injury:
- Thumb spica brace
- Activity modification
- Orthopedic surgery talk for elective ligament repair or reconstruction can be required with a complete rupture.
- Physical or occupational therapy is beneficial to post-operative to improve range of motion and power and to help in resuming ADL activities
Thumb collateral ligament repair or reconstruction?
The collateral ligaments of the thumb may be harmed most repeatedly during playing sports when the thumb is sprung out from the fingers during a history of fall or from an incredible force for example a ball, bat, racket, or fellow player. When the ulnar collateral ligament is injured, it is generally referred to as “gamekeeper’s thumb” or “skier’s thumb”. Injury to the ulnar or radial collateral ligament injuries can results in instability and swelling around the thumb’s metacarpal joint.
Treatment relies on a number of elements:
Count on the severity of the ligament is impaired (whether it will be a partial tear, large avulsion, full tear, or Stener lesion); Whether it is radial collateral or ulnar collateral ligament trauma Timing of display to a professional(for example if the patient has a full tear and waits for more than a few weeks post-injury to see a specialist, then a direct repair might not be appropriate, and the patient may require a reconstruction).
With the late exhibition, the surgery would probably concern the reconstruction of the ligament with the help of using a slip of a tendon from the wrist (commonly the palmaris longus). ulnar collateral ligament injury, with pure ligamentous injury (left) and bony avulsion type injury (right)
Post-operative rehabilitation (developed in convergence with Melbourne Hand Therapy) On the day of surgery, fingers may sense a feeling of numbness or tingling. This is because of the drug. Patients can try to move their fingers, the tip of their thumb, and their wrist (if able) before discharge from the hospital.
Post-surgery, the forearm, and hand will be wrapped and in a plaster cast. These must not be drawn. The bandage must be maintained neat and dry. To reduce the swelling, hands must be raised to heart level.
One week post-surgery: At this phase, a hand therapist will terminate the post-operative dressing and seat a customized thermoplastic splint that fits your thumb over the hand. This splint will stay the whole duration for approximately four weeks following the surgery.
The hand, with the thumb, completely protected within the cast, can be utilized for ADLs, for example, eating, writing, cloth donning and doffing, and grooming. Hefty lifting, or bearing items with the injured hand should be evaded.
4 weeks after surgery: The cast can be terminated for daily basic hygiene activities and light thumb activities (actives only). These activities contain opposing the thumb to each digit of the hand, thumb extension or abduction, and complete wrist movement.
At this phase, patients must be instructed to wear their splint part-time. For example, it can be removed when serving sedentary tasks (for example seating down at the computer or watching TV). At this moment, scar massage will initiate.
6 weeks after surgery: Further weaning out of the splint will occur. Relying on the degree of strength and stiffness, the splint can only be needed when out and about.
If more pliant splints were utilized previous to surgery, these must be brought to a hand therapist to consider whether they can return thermoplastic splints. Softer splints are secure for operating active tasks at this phase
Driving after surgery: An automobile-like car should be able to be safely managed, and involved in a crisis condition, before it is secure to resume driving.
This typically happens about the 4-to-6-week post-surgery mark, when the thermoplastic splint has been terminated. Please do not drive until instructed by Kemble or a hand therapist that it is secure to do so.
FAQ
Cast or splint immobilization of the thumb MCP joint is used for a duration between 4 to 6 weeks permits a period for the torn ligament to relax and recover in an optimal status, and releases stress leading from movement during ADL activities.
The quick reply to that question is normally yes, predominantly immediately following the injury; however, the right quantity of activity and exercise can really encourage recovery and healing from injury
While a ripped ligament can recover naturally as time passes, it is most useful to pursue a medical alert to verify that the affected area recovers accurately without a lot of extreme scarring.
Many LCL injuries cases can be recovered at home with:
Rest and rescue your knee.
Cryotherapy or a cold pack.
Covering your knee with an elastic bandage (compression).
Supporting up (elevating) your knee.
Anti-inflammatory medicine.
STRAIN, SPRAIN, OR LIGAMENT STRAIN: you totally require these fundamental oils:
Helichrysum italicum essential oil.
Katrafay essential oil.
Field mint basic oil.
Lemon eucalyptus vital oil.