Supraspinatus tendonitis
Table of Contents
What is supraspinatus tendonitis?
Supraspinatus tendonitis is a common problem present in the shoulder, also known as “Shoulder Impingement Syndrome” or “Painful Arc Syndrome”.
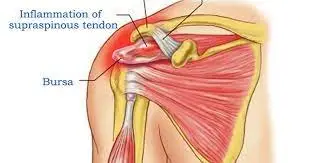
The supraspinatus muscle is a soft tissue structure present in the shoulder that is part of the rotator cuff muscles; this also includes the subscapularis, teres minor, and infraspinatus muscles. It attaches at the top of the scapular (posterior shoulder), then runs underneath the clavicle and acromioclavicular joint to attach at the top of the upper arm (humerus) on the greater tuberosity.
The function of the supraspinatus muscle is to raise the arm outwards from the side, clinically known as ‘abduction.’ It also plays a role in external rotation and resisting gravitational forces on the glenohumeral joint. When the tendon becomes inflamed or irritated, it is termed tendonitis.
Shoulder impingement syndrome is the most common problem with 1 in 5 people having symptoms at some point in their lives.
Supraspinatus Tendonitis symptoms may come on abruptly after an injury, or build up slowly on and off over years with no obvious cause.
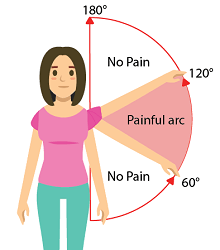
There is a classic sign of supraspinatus tendonitis:
There is a painful arc when moving the arm between 60-120 degrees of abduction as the tendon gets compressed against the bone in that range.
Symptoms of painful arc syndrome typically present in middle age, most frequently between the ages of 45-65.
Generally, supraspinatus tendonitis is an overuse injury caused by repetitive friction on the tendon, but it can be caused by any injury in the shoulder, instability, or shoulder impingement.
Related Anatomy:
The shoulder joint consists of three bones: the humerus, scapula, and clavicle.
The head of the humerus articulates with the glenoid cavity of the scapula to form a ball-and-socket joint.
The supraspinatus muscle is located on the back of the shoulder, forming part of the rotator cuff present in the shoulder.
The rotator cuff consists of Supraspinatus, Infraspinatus, Subscapularis, and teres minor. The rotator cuff covers the head of the humerus and keeps it in place. These muscles help to lift and rotate the arm.
- Origin: Muscle origin from Supraspinous fossa of the scapula
- Insertion: Muscle inserts into the Greater tubercle of the humerus
- Innervation: nerve supply by Suprascapular nerve (C5-C6)
- Function: It helps in the abduction of the glenohumeral joint; also assists the rotator cuff in stabilizing, controlling, and moving the shoulder; assists in preventing shoulder subluxation.
Causes of Supraspinatus tendonitis:
The Supraspinatus muscle has the greatest stress force during the abduction.
Injury to the supraspinatus muscle is due to the following causes:
Traumatic events
Degenerative tears in the muscle
Risk inpatients such as:
- Heavy laborers
- Overhead labor
Degenerative tears may occur after a specific injury including lifting any object, shoulder dislocation event, falls, or other unexpected arm loading events.
Lifting a shoulder overhead or moving the arm above the head may cause pinching of supraspinatus tendons of the rotator cuff between the upper part of the arm bone and the acromion. This pinching of this tendon is called impingement.
Repetitive activity: It occurs due to repetitive use of the shoulder joint. Due to repetitive movement, it can cause the supraspinatus tendon and other neighboring rotator cuff tendons to become inflamed such as the biceps tendon.
Poor posture: If shoulders are protracted forward from poor posture then the supraspinatus tendon can get blocked under a bony prominence called the acromion process. Due to this, there is continuous compression which leads to inflammation and irritation. This condition is also termed subacromial supraspinatus impingement or shoulder impingement syndrome. There are three sites in the shoulder where the tendon can become impinged:
- Under the acromion
- On the glenoid rim
- Under the coracoacromial ligament. The coracoacromial ligament attaches between the acromion process and the coracoid process of the scapula.
Direct blow: If a person falls onto or is hit on the shoulder then it can directly inflame the supraspinatus tendon and affect the function of the shoulder joint.
Ligament laxity: When the ligaments around the shoulder are weak and lax, it causes the shoulder joint to become unstable. The rotator cuff tendons then have to work harder to stabilize during movement, and as a result, can develop tendinitis.
Signs and symptoms of Supraspinatus tendonitis:
- Pain increases with overhead reaching.
- Pain is felt after frequent repetitive activity at, or above the shoulder.
- The patient feels weakness in the shoulder joint
- The patient may have pain from resisted abduction and forward flexion, especially with pushing and overhead movements.
- The patient has difficulty sleeping at night due to pain in the shoulder, especially when lying on the affected side of the shoulder.
- The patient may have difficulties with simple movements, such as brushing hair, putting on a shirt or jacket, or reaching the arm above shoulder height.
- The patient has a limited range of motion in the shoulder. Position such as Shoulder flexion, abduction, and rotation.
- The patient may have a referred pain in ar.
- The patient may have a former shoulder trauma.
- The patient may have tenderness over the affected arm.
- It may have to swell around the affected tendon.
- The patient may have shoulder limited mobility.
- The patient may have a burning sensation in the shoulder.
- Dull ache in the shoulder that increases on elevation, and overhead activity.
- Decrease in the strength of muscle.
- The patient may have pain when trying to reach behind the back
- Stiffness in the joint
- Tightness in the capsule
- The patient may have triggered pain while lowering or raising your arm
- Inflammation in the joint
- The patient may have difficulty in dressing.
- The shoulder may be warm in the injured area at all times and there may be fullness anterolaterally. Further, the shoulder has a painful arc between 70° and 120° of abduction.
Supraspinatus tendinopathy is usually consistent with anterior instability causing posterior capsule tightness.
The main problems that patients with supraspinatus tendinopathy complain of are: pain, inflammation, decreased ROM, strength, and functional activity
Diagnosis:
Yet the diagnosis of this condition is usually clinical, but imaging can be a useful method to diagnose the condition. Imaging such as X-ray, and MRI.
X-rays: Shoulder x-rays can show calcifications in the rotator cuff tendons and in the bursa. In chronic cases of this condition, there may be degenerative changes, such as cystic or sclerotic changes at the greater tuberosity and decreased humeral head-acromion distance, secondary to the upward movement of the humeral head. In acute calcific tendinopathy, calcifications may be uneven, fluffy, and ill-defined.
Dynamic ultrasound can reveal thickening of the subacromial bursa and impingement during the abduction movement.
Ultrasonography
Magnetic resonance imaging (MRI) can be done.
Diagnosis is based on the appearance of the rotator cuff tendons (grading system) and the presence or absence of signs indicating the involvement of the subacromial bursa and subacromial–subdeltoid plane.
Diagnosis by physical examination:
The shoulders are observed for symmetry, localized swelling, and muscle atrophy. There may be the presence of a tender point below the acromion process and over the greater tuberosity. Inward rotation of the shoulder can help in the palpation of the supraspinatus insertion on the greater tuberosity. The most important clinical tests are as follows:
Painful arc Testings:
1. Neer’s sign:
The Neer’s Sign can be observed by performing the Neer’s test.
Procedure: The test is designed to test for impingement of the muscles that make up the rotator cuff.Position: Standing with the elbow flexed
Test: Stand fully straight but relaxed.
The doctor will rotate and abduct the affected arm making note of the range of motion.
Once movement is completed, if the Neer’s sign is positive, the patient will report having pain on the lateral (side) portion of their shoulder, as well as their anterior (front) portion.
2. Hawkin Kennedy Test:
Position: The arm is supported in 90-degree shoulder and elbow flexion
Test: Forearm pushed downwards to internally rotate the shoulder. The test is repeated bringing the arm into different positions of adduction across the body
Positive Result: A patient has pain in the shoulder
Supraspinatus challenge test/“The Empty Can” sign/Job‘s test:
Position: Both arms raised to 90 degrees abduction and 30 degrees forwards flexion, thumbs pointing to the ceiling
Test: Rotate arms so thumbs point down. The examiner pushes down through forearms while the patient resists the movement
Positive Result: Pain in the shoulder
3. Drop arm test
4. Impingement test
Treatment of Supraspinatus tendonitis:
The treatment to manage supraspinatus tendinopathy depends on the cause of the pathology.
At first, conservative treatment is preferred. Conservative treatment involves physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), cold pack treatments, and resting.
Corticoid injections can also be used in addition to physiotherapy. Surgical intervention can be another solution if there is no improvement after 3-6 months of conservative treatment.
Rest: Rest to the affected limb.
ice massage: It will reduce pain and inflammation.
Medical Management:
NSAIDs (nonsteroidal anti-inflammatory drugs) may be the first choice for mild to moderate pain if there are no contraindications to these agents. A drug is given for 7-14 days to relieve the pain associated with tendinitis.
Moderate to unbearable symptoms may require a local subacromial corticosteroid injection.
Surgical Treatment:
The major indications for surgery are ongoing pain, loss of function of the shoulder, failure to respond to conservative therapy for 3 months or more, or evidence of an acute tear in a younger patient.
Surgical approaches include calcium deposit resection, with or without subacromial decompression, bursal resection, and acromioplasty, using either arthroscopic or open methods. It is also possible to cut off the coracoacromial ligament to enlarge the space between the acromion and humerus. This can cause instability, but we can repay it with some training in the rotator cuff. With physiotherapy, it takes patients up to 4 months to heal. The goal of surgery is to obtain pain relief, increased range of motion, and increased power.
Abursal resection: Removement of the subacromial bursa.
Acromioplasty: Generally, there is the removal of a small piece of the surface of the acromion process that is in contact with a tendon causing, by friction, damage to the surrounding tissue.
Physical Therapy treatment in Supraspinatus tendonitis:
Painful arc syndrome can be treated by a physical therapist. The doctor will fully assess your shoulder and identify the cause which may be contributing to your shoulder problem
The main goal in the acute phase (initial phase) is to relieve pain, and inflammation, prevent aggravation of pain, reduce muscle wasting and normalize the arthrokinematics of the shoulder girdle. A period of rest should be most important in order to avoid further irritation and shoulder discomfort.
- Modalities: Ultrasound, Cryotherapy, and Electrical stimulation for muscles can provide temporary relief in the acute phase.Ultrasound: To help reduce inflammation and realign tendon fibers
- Cryotherapy, soft tissue techniques, and wearing a sling and taping technique are some other techniques to decrease pain.
- Proper home exercise programs should also be taught in convergence with proper ergonomics.
- Posture Work: To improve posture also helps in reducing pain.
- Stretching Exercises:
- To reduce the muscle tightness
- Shoulder Stretches: Stretching of muscles reduces the tension on the muscles
- Upper Back Stretches: reduce pain and stiffness
- Exercises:
To enhance strength and flexibility of the shoulder.
Scapular Stabilization Exercises: Improves scapular strength
Rotator Cuff Exercises: Improves shoulder strength
Early management for this condition includes avoidance of repetitive movements that aggravate the pain in the shoulder.
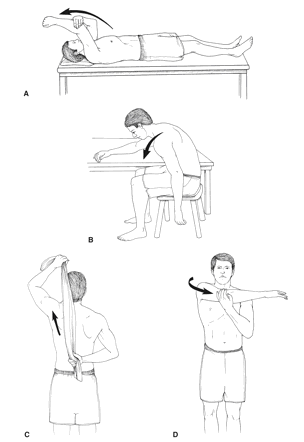
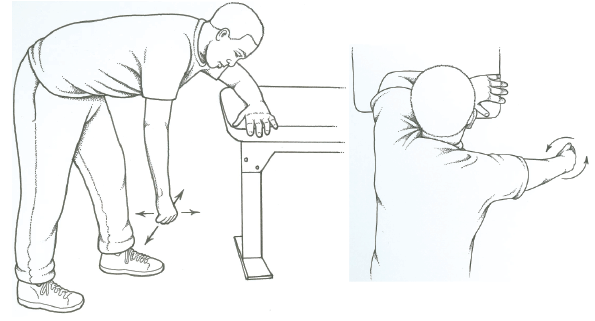
Gentle range-of-motion exercises:
Range of motion of shoulder joint. Initiate with shoulder passive movement. Followed by exercises, such as:
Codman’s pendulum exercises, To maintain range of motion and prevent the development of a frozen shoulder. Once the pain has been decreased, joint mobilizations, massages, muscle stretches, and active-assisted and active exercises are needed to improve the ROM more.
Active-assisted mobilizations: These can be done by the patient self by using an exercise bar. Patients can also use a rope, stick, and pulley, In this way, the unaffected arm helps to pull the affected arm into anteversion.
As an active assisted exercise person can do, a physiotherapist works on resistance exercises for strengthening shoulder muscles.
Strengthening exercises: Strengthening of external and internal rotators, biceps, deltoid, and scapular stabilizing muscles. Strengthening all these muscles will keep the shoulder joint more stable and powerful and prevent further injuries. Eccentric exercises will also be more efficacious than concentric exercises. Strengthening exercises are done with the help of theraband, dumbbells, and weight cuffs of different weights as progression is needed.

Summary:
Supraspinatus tendinopathy is an ordinary condition of shoulder pain in athletes that participate in overhead sports (handball, volleyball, tennis, baseball). In most cases, this tendinopathy is caused by an impingement of the supraspinatus tendon on the acromion as it passes between the acromion process and the humeral head. Pain and a decrease in range of motion, strength, and functionality are the main complaints by patients that accompany this injury and should be addressed in physical therapy.
There is enough evidence to prove that physical applications such as ultrasound, cryotherapy, hyperthermia, transcutaneous electrical nerve stimulation(TENS), and extracorporeal shock wave therapy have a beneficial effect on the recovery of supraspinatus tendinopathy. But we have to remember that it is very important to use these methods as an adjunct to physical therapy including increasing ROM, strength training of the rotator cuff muscles, and other shoulder stabilizers.
FAQs:
What causes supraspinatus tendonitis?
Supraspinatus tendonitis develops when there is repetitive movement or friction occurring on the tendon or it is repeatedly squashed or “impinged” in the subacromial space. This leads to inflammation and gradual degeneration of that tendon.
What are the symptoms of supraspinatus tendonitis?
Symptoms of supraspinatus tendonitis are as follows:
Pain occurs when raising the arm forward, sideways, or above shoulder height.
Repetitive activities that involve shoulder movement.
A burning sensation occurs in the shoulder.
Weakness in the shoulder when lifting up an object or pushing a door open.
Disturb in sleep due to the pain.How do you treat supraspinatus tendonitis?
Supraspinatus tendonitis treatment involves physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), cold treatments, and resting. In addition to physical therapy, corticoid injections can also be used. Surgical treatment can be the solution if there is no improvement after 6 months of conservative treatment.
How painful is supraspinatus tendinosis?
Supraspinatus tendonitis is painful because the tendon is structurally intact and not torn, just strength is generally unaffected but limited by pain. Some patients have pain that radiates into the neck, back or upper arm due to fatigue in shoulder muscles. Some patients report pain when a person tries to reach for the back pocket.
Does supraspinatus tendinosis require surgery?
Treatments for supraspinatus tendonitis include anti-inflammatory medicine (NSAIDs), cold, and physical therapy. If those treatments do not work, the doctor may recommend surgery.