
Scapula Bone
Table of Contents
Introduction
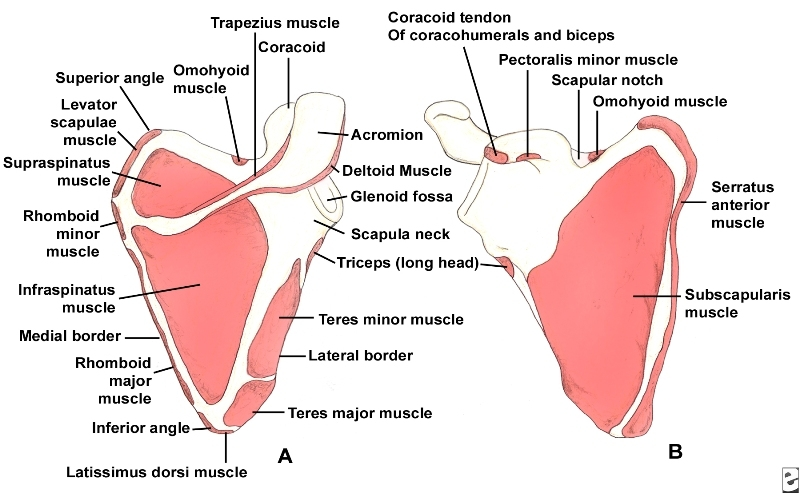
The scapula (Latin shoulder blade) is located on the posterolateral aspect of the thoracic cage.
The scapula has two surfaces, three borders, three angles, and three procedures.
The scapula is again understood as the shoulder blade. It articulates with the humerus at the glenohumeral joint, and with the clavicle at the acromioclavicular joint. the scapula connects the upper limb to the thorax.
It is a triangular, flat bone, which serves as a site for attachment for many muscles.
In this article, we discuss the anatomy of the scapula – its bony landmarks, articulations, and clinical importance.
Side determination
The lateral sidewards or glenoid curve is big and accepts the glenoid cavity.
The convex character bearing the spinous process should be directed dorsally while the indented character should be directed ventrally.
The dorsal character is convex and is divided by the triangular spine into the supraspinatus fossa and infraspinatus fossa Costal texture is indented.
The sideways most thick structure functions from the glenoid cavity above to the inferior angle descending.
Features
Two surfaces
Costal surface:
Also understood as ventral surface or subscapular fossa Proposes a comprehensive concavity (orchestrated medially and forwards) Medial two-thirds of the fossa are marked by several oblique ridges; that runs lateral ward and upwards.
The sideward third of the fossa is smooth. A close ridge connects the sideward boundary Nearly rod-like Fronts as a lever for the action of S.A. in the above abduction of the component.
Dorsal surface :
Arched from above downwards.
Gives attachment to the spine of the scapula which divides the surface into two unequal parts: supraspinatus fossa and infraspinatus fossa. Two fossae are connected by the supraglenoid notch, situated lateral to the root of the spine.
Supraspinatus fossa: Smaller of the two Concave, smooth, and broader Medial two-thirds give origin to the supraspinatus
Infraspinatus fossa: Much larger Superficial concavity at its upper part Centre presents a prominent convexity.
Medial two-thirds provide a source to the Infraspinatus muscles.
Three border
Superior border :
Shortest and thinnest, most irregular, Concave, Extends from the medial angle to the base of the coracoid process.
Roughly the core of the coracoid procedure, it suggests in the suprascapular notch.
Axillary border or lateral border:
Thickest, Commences overhead at the more defective margin of the glenoid cavity.
Inclines transversely lowered and rearwards to the inferior curve.
At the upper end, it presents the infra glenoid tubercle Vertebral border or medial border: Longest, Extends from the superior angle to the inferior angle.
Three angles
Superior angle:
Started with the junction of the superior and vertebral boundaries. Thick, smooth, rounded.
She inclined relatively lateral ward Covered by the trapezius muscle.
Inferior angle:
Thick and rough.
Formed by the union of the vertebral and axillary lines.
Covered by the Latissimus dorsi muscle.
Moves forwards around the chest when the arm is abducted.
Lateral angle:
Also known as the glenoid angle.
The thickest part of the bone.
Receives the glenoid cavity or fossa.
Directed forwards, laterally, and slightly upwards.
Three process
Spine or Spinous process:
Triangular part of a bone.
Three borders and two surfaces.
Separates on the dorsal character of the scapula into the supraspinous and infraspinatus fossa.
The posterior border is called the crest of the spine, Crest has upper and lower lips.
The lateral border is the shortest, slightly concave, thick, and round.
Acromion process:
Large and relatively triangular.
Has two borders, medial and lateral.
The sideward boundary stands stuffy and uncommon.
The medial border is shorter than the lateral and concave.
Two consistencies, outstanding and insufficient.
The superior surface is directed upwards, backward, and lateral ward; convex, rough.
The inferior surface is smooth and concave. A part for the clavicle.
Coracoid process:
A facet for the clavicle. Thick curved process.
Attached by an overall base to the upper part of the neck of the scapula.
Directed forwards and slightly laterally.
Blood Supply and Lymphatics
The scapular blood supply is complex due to its function and role as a necessary component of the shoulder joint and the necessity for adaptability. It is largely provided by an anastomosis between the axillary artery and subclavian artery learned as scapular anastomosis.
Contributory routes to this anastomosis are the dorsal scapular artery, the suprascapular artery, the deep scapular artery, the circumflex scapular branch of the subscapular artery, and the medial anastomoses with the intercostal arteries. Scapular anastomosis permits collateral blood flow when lying supine and when using the shoulder in its group of positions.
The venous drainage of the scapula is largely achieved by the axillary vein, the suprascapular veins, and numerous small and highly variable anastomotic tributaries.
The lymphatic drainage from the right scapula empties into the right lymphatic flue and the thoracic flue from the left scapula. The lymph nodes associated with the scapula possess the axillary and the supraclavicular lymph nodes.
Nerves
The nerves to the scapula form the dorsal scapular, upper and lower subscapular, and suprascapular nerves, which originate from the brachial plexus at the anterior ramus C5 root, the posterior cord, and the superior trunk respectively. See the “Muscles” section downward for more details regarding specific muscle innervations.
Attachments of Scapula
Muscles
Subscapularis: medial two-thirds in the scapula subscapular fossa.
Supraspinatus: medial two-thirds of the supraspinatus fossa including the upper spine surface.
Infraspinatus: medial two-thirds of the infraspinatus fossa including the lower spine surface.
Deltoid muscle: more inferior boundary of the crest of the spine and from the sidewards boundary of the acromion.
Biceps brachii: long head; supraglenoid tubercle, short head; lateral part of the tip of the coracoid process.
Coracobrachialis: medial part of the pinpoint area of the coracoid approach in a scapula.
Triceps brachii: long head from the infra glenoid tubercle.
Teres minor: dorsal surface, upper two-thirds, lateral border.
Teres major: dorsal surface, lower one-third, lateral border.
Omohyoid: suprascapular notch Insertion.
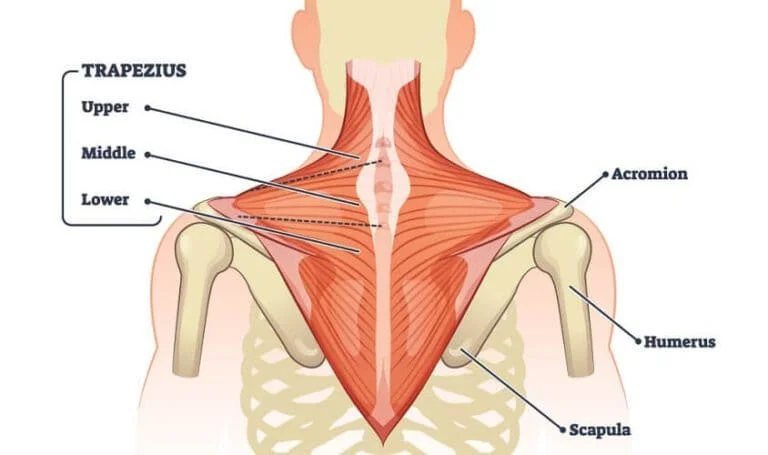
Trapezius: upper border of the crest of the spine and medial border of the acromion process.
S.A. (serratus anterior): medial border of the costal surface.
Pectoralis minor: medial border and the superior surface of the coracoid process.
Levator scapulae: dorsal aspect, medial border, from the superior angle to the root of the spine.
Rhomboideus minor: medial border, dorsal aspect, opposite the root of the spine.
Rhomboideus major: medial border, dorsal aspect, between the root of the spine and the inferior angle.
Ligaments
Glenoid labrum: margin of the glenoid cavity.
The capsule of the AC joint: margin of the acromion facet.
Coracoacromial ligament: lateral border of the coracoid process, medial side of the tip of the acromion process.
Coracohumeral ligament: the root of the coracoid process.
Coracoclavicular ligament: coracoid process.
Suprascapular ligament: bridges across the suprascapular notch.
Bursae
There are 2 main bursae:
Scapulothoracic Bursa: located between the serratus and the thorax.
Subscapularis Bursa: located between the subscapularis and the serratus.
Biomechanics of Scapula
The scapula upwardly turns in the frontal plane, posteriorly tips in the parasagittal plane, and externally rotations in the transverse plane during functional elevation. Scapular control is important to scapulohumeral coordination. Posterior tilting is responsible for humeral support during the acromiohumeral part of shoulder elevation.
Fung et al discovered that scapular upward rotation and retraction are greatest during abduction elevation when likened to flexion elevation. They also located that posterior tilting was most prominent during flexion elevation. Any disorder in this rhythm can decrease scapulothoracic motion and can be associated with fatigue, impingement, fluctuation, and limits in height.
Ossification of Scapula
Ossification compromises of the pectoral girdle can be divided into individually of the three bones that constitute it: clavicle and scapula bone to the proximal humerus.
Ossification centres of the clavicle
lateral end: 5 weeks in utero
medial end: 15 years
Ossification centers of the scapula
body: 8 weeks in utero
coracoid process (two centers): 12-18 months
glenoid: 10-11 years
inferior angle: 14-20 years (puberty)
acromion (three centers): 14-20 years (puberty)
medial border: 14-20 years (puberty)
Ossification centers of the proximal humerus
diaphysis (shaft): 8 weeks in utero
head: 1-6 months
greater tubercle: 1 year
lesser tubercle: 3-5 years
Clinical Importance
Scapulothoracic dysfunction
Numerous standard structure exists in winging of the scapula. Surgery to the axilla, e.g. in the possibility of a case mastectomy, can occasionally exist associated with impairment to the extended thoracic nerve innervating in the serratus anterior muscle. As a result, the inferior angle of the scapula protrudes backward and can easily be seen through the skin of the patient due to the unopposed action of the trapezius, levator scapulae, and rhomboid muscles.
Scapulothoracic is the sin of political instability another result of injury to the dorsal scapular nerve supplying the rhomboid muscles, and the spinal extra item good nerve to the trapezius. Damage part to the dorsal scapular nerve results in winging of the scapula which is milder than what occurs with an impaired long thoracic nerve. Injury to the spinal nerve from the neck region, irradiation, or laceration leads to a depressed and rotated scapula due to the action of the serratus anterior muscle.
Scapular dysplasia
Somebody has an abnormal morphology of the scapula which can one or the other be primary or acquired, secondary to obstetric brachial plexus palsy. The scapula is the glenoid/coracoid block, spine/acromion block, and blade. first, the dysplasia is due to incomplete ossification of the glenoid and leads to bilateral anatomical changes the glenoid is flattened and elongated leading to clicking, Morphological changes in the scapula can also be seen in infants featuring a brachial connection injury at the time of the delivery due to abnormal development of the cartilage of the posterior glenoid.
It the commonly characterized by impaction of the fetal shoulder against the antenna of the maternal symphysis pubis. Posteroinferior glenoid dysplasia can appear in teenagers with a record of shoulder pain and is featured by a silent dislocation of the glenohumeral joint as the humeral head moves posteriorly when the arm is raised in adduction and internal rotation. This is occasionally associated with a feature of a dimple on the back of the involved shoulder.
For the scapula to smoothly glide over the chest wall (termed the scapulothoracic joint) several muscles lie between the ribs and scapular to facilitate this. Also, a person is assisted which helps cushion the tissue and decrease. There are two major bursae at the scapulothoracic joint: scapulothoracic (or infraspinatus; between the serratus anterior muscle and chest wall) and the subscapular bursae (between the subscapularis muscle and serratus anterior muscle).
Snapping scapula syndrome
Snapping scapula syndrome is when there is an irregularity at the scapulothoracic joint which guides to non-smooth representation. The two considerable common causes are either lesions or when the bursae evolve inflamed, which is termed scapulothoracic bursitis.
The multiple typical casualties of lesions exist due to osteochondroma, a delicate cartilage tumor that can induce lesions on the anterior character of the scapula. Scapulothoracic bursitis exists often due to repeated motions of the joint usually due to an over-the-head component movement.
scapular winging
The scapula, or shoulder blades, are flat bones that attach the upper arm to the collar bone. When they come out of location, it can cause scapular winging.
Winging of Scapula is a rare condition that can be very painful.
This essay will examine the possible causes of scapular winging, symptoms, and treatment methods.
A common reason for scapular winging is nerve injury. It may involve one of three major nerves in the shoulder.
The dorsal scapular nerve holds the rhomboid muscles.
The spinal accessory nerve holds the trapezius muscle.
The long thoracic nerve holds the serratus anterior muscle. Injuries to these nerves or covering muscles can result from overuse of the shoulder, back, or neck.
FAQ
The scapula is accountable for several indications which are integral to daily movement and smooth upper extremity motion. Protraction and retraction of the scapula help with the action of the pectoral girdle and chest muscles both ahead and back, respectively.
The source of the backbone of the scapula is the considerable medial segment of the scapular crest. It is termed the “triangular location of the divide of scapula”, established on its triangular constitution blessing it a different observable form on x-ray photographs.
Particularly, the muscles power of the scapula position pursues:
Serratus Anterior: The serratus anterior muscle is a necessary scapular stabilizing muscle.
Rhomboids: The rhomboids (major and minor) position to stabilize the medial boundary of the scapula.
Trapezius (Upper/Middle/Lower): Levator Scapulae.
It stands as the greatest prostrate lengthy bone in our body. The clavicle incorporates the shoulder girdle with the shoulder dagger. the location and structure give information regarding body alignment. This justifies the name “beauty bone”.
At rest, the scapula is positioned approximately horizontally, with 35° of internal rotation and 10° anterior tilt. During shoulder height, most experimenters approve that the scapula tilts posteriorly and rotates both upward and externally.

13 Comments