Retrolisthesis
Table of Contents
What is a Retrolisthesis?
Retrolisthesis occurs when a vertebra slips beneath or along a disc in the back, causing joint dysfunction.
A retrolisthesis happens when a vertebra slips backward, and spondylolisthesis occurs when a vertebra slips forward. Back pain is frequently caused by retrolisthesis in the neck, shoulder, or lumbar areas of the back. Movements in each direction are at least two millimeters (mm).
Retrolisthesis can happen, however it is less common in the thoracic and middle regions of the spine.
The Spine: Anatomy and Function
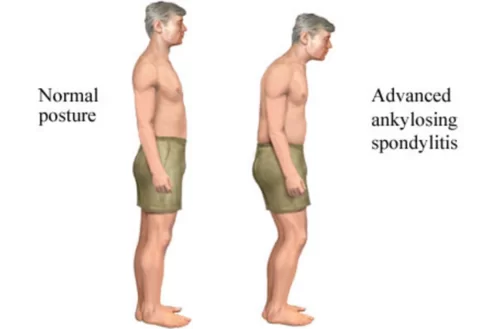
The spine is naturally curved in each part, giving it a straight aspect when viewed from the front or back and a soft ‘S’ shape when viewed from the sides.
The natural and healthy curves of the spine make it stronger, more flexible, and better able to absorb and distribute mechanical stress equally during movement along the spine.
The spine is devided into 3 parts:
- cervical spine (neck)
- thoracic spine (middle/upper back)
- lumbar spine (lower back)
Each of the natural curves of the spine is dependent on the health of the others. When a healthy curve disappears, the spine often responds by putting in compensatory curves, which can affect the biomechanics of the entire spine.
The spine is made up of vertebrae (bones) stacked on top of one another in a straight and neutral alignment, allowing the spine to function normally, with its structures working together to maintain those natural spinal curves and keep the spine aligned.
An intervertebral disc exists between adjacent vertebral bodies; the discs of the spine are frequently the first spinal structures to show signs of degeneration. This is partially due to the several crucial functions they perform for the health and functionality of the spine.
The intervertebral discs are made up of two parts: an inner gel-like nucleus and a strong outer annulus.
Retrolisthesis Types and Grades:
Based on the position of the vertebra concerning the next vertebra, retrolisthesis is classified into three types:
- Complete retrolisthesis: One vertebra slips backward about the positioning of both vertebrae above and below.
- Partial retrolisthesis: One vertebra shifts backward to a spinal segment about the positioning of either vertebra above or below.
- Stair-stepped retrolisthesis: One vertebra goes backward in relation to the vertebra above, but moves ahead of the one below.
The percentage of backward displacement of the intervertebral foramina affects the grade of retrolisthesis. The grades are also helpful in determining the instability of the surrounding joint.
- Grade I: 25%
- Grade II: 25%-50%
- Grade III: 50%-75%
- Grade IV: 75%-100%
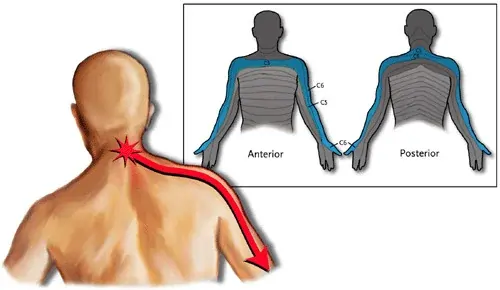
Signs and symptoms of retrolisthesis:
The symptoms vary depending on your overall health, the location of the slippage, and which nerve tissues, spinal joints, and other tissues were damaged.
Among the signs and symptoms are:
- Uncomfort in one place on your back
- A twisted spine or a bulge in your back
- A restricted range of motion
- Backache
- Other types of discomfort in the displacement area
- You may also experience numbness, tingling, or a sharp, pinched pain in the following areas:
- Hips
- Thighs
- Legs
- Buttocks
- Neck
- Shoulders
- Arms
Causes:
When the space between the vertebrae reduces, this is referred to as retrolisthesis. This can occur when the discs between the vertebrae shrink. Scientists are unclear what causes the discs and space between the vertebrae to narrow.
However, they believe the following reasons may be causing this shrinkage and resulting in retrolisthesis:
- Degenerative spinal disorders
- Arthritis
- Disabilities that occur at birth
- Spine injuries or injuries near the spine
- Muscle weakness in the abdomen and around the spine
- Infections of the blood or bones
- Osteoporosis
- Deficiencies in nutrition
Diagnosis:
A doctor starts by assessing a person’s overall health as well as the symptoms they are experiencing. If a doctor identifies retrolisthesis after the examination, he or she may recommend a lateral X-ray. Because it is impossible to identify retrolisthesis while the patient is lying down, a lateral X-ray is conducted while the patient is standing.
The X-ray will be examined by a doctor, who will most likely draw many lines on it to compare the positions of the vertebrae and determine how far the vertebrae have moved out of position. Any slippage greater than 2 millimeters is considered retrolisthesis.
- The X-ray can also highlight any additional signs that may indicate retrolisthesis. Additional indicators may include:
- Calcified arteries around the vertebrae
- Reduced disc heights
- Bone spurs
- Gas trapped between vertebrae
The intervertebral discs support the spine’s flexibility, act as shock absorbers for the spine, and cushion adjacent vertebrae to lessen friction during movement.
Disc degeneration can cause a variety of disc disorders, including desiccation, bulging, and disc herniation (particularly lumbar disc herniation).
So any change in the spine, including retrolisthesis, is likely to influence the discs.
What Is the Treatment for Retrolisthesis?
During retrolisthesis treatment, inflammation, and pain should be decreased. Different therapy options are used depending on the severity of the problem and how other tissues and discs may be damaged.
Surgical Treatment:
Surgery is only required when non-surgical treatments are unsuccessful. Before recommending surgery, the orthopedist and physician may assess the risk of long-term spinal and neurological damage. The benefits of spinal surgery include reducing slippage, pain, and instability and avoiding or reversing any neurologic damage.
Non-Surgical Treatment:
Repositioning
The incorrect vertebral posture in retrolisthesis is addressed to eliminate inappropriate stress on the soft tissues of the spine and nerve discomfort.
Robb myofascial release
The myofascial release improves stability by restoring normal muscle tone. Myofascial release increases the range of motion by relaxing tight muscles, increasing vascular and lymphatic circulation, and causing the muscular stretch reflex.
Nutrition
Vitamin and mineral supplements are recommended to help in repairing soft tissue injury and maintaining spinal posture. Taking copper, glucosamine, manganese, vitamin C, zinc, and water is advised. Proteins and amino acids, for example, are also beneficial to tissue regeneration and health.
Microcurrent therapy
Microcurrent therapy has the potential to reduce swelling and inflammation, mask acute pain, release muscle trigger points, regulate pain, help tissue repair, and increase soft tissue regeneration.
Water therapy
Water therapy exercise programs relieve low back or neck pain, condition and strengthen muscles to help avoid future back pain recurrences, and are especially beneficial when a land-based exercise program is not possible due to the intensity of pain, reduced bone density, disability, or other factors.
Other treatments
Smoking should be avoided since it might lead to increased joint degeneration and injury. Weight loss is advised in order to relieve pressure on the vertebrae.
Physical Therapy Treatment:
Mobility exercises
The greatest contributors to the mechanical efficiency of the spine and the entire body are mobility exercises. Apophyseal joints of the spine require mobility or movement to enable nutrition and prevent articular cartilage degradation.
Flexibility exercises
Flexibility goal at improving disc nutrition. Gentle and gradual heat and controlled rapid stretching improves flexibility. Elongation exercise must be initiated, but biomechanical characteristics of collagen fibers must be kept in mind. Rotation and sagittal motion must be included in flexibility exercises.
Strengthening exercises
Strengthen deep abdominal muscles, particularly the transversus abdominis and quadratus lumborum.
Effects of exercise
Exercise also raises the level of endorphins in the blood and cerebrospinal fluid, which enhances nutrition to joint cartilage, including intervertebral discs, increases skeletal muscle oxidizing capacity, improves neuromotor control and coordination, and promotes feelings of well-being by increasing alpha wave activity, which causes central and peripheral relaxation and a reduction in muscle tension. Endorphine has been shown to have a considerable pain-relieving impact as well as to lessen the symptoms of despair and anxiety.
Therapeutic lifestyle changes
Patient education about the condition and the list of precautions play an important role. Changes in posture and activity have an impact on intradiscal pressure. Sitting with the hips and knees flexed or leaning forward should be avoided for acute disc injuries; instead, the lumbar spine should be supported with the trunk inclined 120° to offer the least strain to the disc. Lifting and bending techniques are demonstrated. Sitting for a bowel movement may result in a significant increase in intradiscal pressure due to the Valsalva maneuver. The patient is taught to sit with a wide base of support, leaning back. It is best to use a higher toilet seat.
Retrolisthesis Exercises:
- Specific exercise protocols:

Walking as an exercise prescription is likely the simplest, least stressful, and most beneficial therapeutic exercise for the lower back. Proper walking involves contralateral arm swing, which results in physiologic trunk rotation at each step. As each functional unit rotates physiologically, the collagen fibers of that layer and, thus, that angulation are expanded, which strengthens them.
- Core exercises:
A strong core helps relieve stress on the spine. Strengthening the gluteal and abdominal muscles decrease pain in the lower back and buttocks.
- Extension exercises:
- Extensive exercises have the following effects:
- Extension exercises help to maintain the spine’s normal physiologic lumbar curve, which allows it to endure axial compression forces and so facilitates lifting loads.
- They improve the motor recruitment, strength, and endurance of the spine and hip extensor muscles.
- Extensors are the primary muscle groups involved in postural retention and eccentric trunk flexion regulation.
- They increase the spine’s mobility.
- They increase tone in the extensor muscles, which is frequently diminished due to the human body’s maximal natural flexion posture.
Extension exercises are of two types:

- Extension to neutral. It involves concentric contraction of the back extensors from a trunk flexion of 40° to 45°. The benefit of this exercise is that it involves eccentric extensor contractions as the trunk returns to its initial position of 40-45° of flexion.
- Exercise for hypertension: In the prone position, the patient stretches the spine beyond the neutral position, resulting in 15-30° of hypertension.
- Hypertension exercise: In a prone, the patient extends the spine beyond the neutral position up to 15-30° of hypertension.
- Spinal exercises:

Active exercises should be done in a controlled, gradual and progressive manner. In the acute stage, the McKenzie protocol has been shown to be useful. To keep the discs, muscles, ligaments, and joints healthy, movement sends nutrients into the disc space and soft tissues of the spine. These workouts also help to reduce disc bulging.
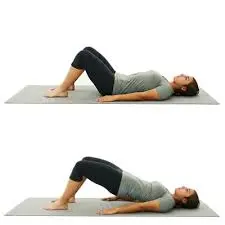
- Pelvic tilts:

Pelvic tilts are a low-impact, lying-down exercise for strengthening the lower back. This exercise helps in the loosening of stiff joints and the relief of pain caused by a range of lower-back disorders, including sciatica and arthritis. The exercise also tightens and strengthens the lower abdominal wall and pelvic muscles. Lie on your lower back and bend your knees. Pull the abdomen in towards the floor and rock the top of the pelvis upward slightly. Hold the tilt for 10 seconds before relaxing.
- Lower back rolls:

If your retrolisthesis has produced moderate to severe placement of the lower vertebrae, you may be unable to do this activity. However, exercise may help with pain relief. According to Capital Health, slowly raise your knees to your chest and clasp your hands behind your knees. Allow your body to roll to the left slowly, then return to the starting position. Rest for a moment before rolling to the right.
- Hip Rolls:
When diagnosed with lower back pain, the hip joints and pelvic region must be strengthened. To perform this Retrolisthesis exercise, stand with your hands on a wall. The left leg should be slightly bent at the knee, with only the ball of the foot touching the ground, while the right leg should be straight and bear the majority of the weight. Now, carefully rotate the left knee outward and then inward. This retrolisthesis practice should be repeated with different legs.
- Posture and ergonomic advice:

The patient must be trained on good posture and ergonomics in order to minimize the recurrence of the condition and to improve functional independence in the future without putting excessive strain on the back structure.
How to Prevent Retrolisthesis?
Although retrolisthesis is not always prevented, there are things you may take to reduce your risk. Try the ideas below.
- Tips for prevention:
- Maintain a balanced diet and weight for maximum bone health and less back strain.
- Pelvic tilt exercises will help you strengthen your core muscles. A strong core reduces back pain.
- Maintain proper posture while sitting and standing.
- Yoga helps to enhance posture, core strength, and back alignment.
- Avoid putting too much weight on your back by hyperextending it.
- Smoking should be avoided. Tobacco use can lead to joint degeneration over time.
How serious is it?
If diagnosed early, the slippage can be stabilized; however, if not treated, it can worsen and lead to problems.
If Untreated, it can cause spinal cord compression or cervical spondylotic myelopathy (CSM), especially in adults over 50.
There may be the following symptoms as the nerves are compressed:
- Neck ache
- Arms and hands numbness and weakness
- Balance and coordination issues
- Impaired mobility
Summary:
Retrolisthesis can be avoided by taking appropriate care of one’s back, which includes regular exercise, a balanced diet, and avoiding dangerous hobbies.
Patients with retrolisthesis typically achieve a full recovery after continuing their doctor’s treatment program. Surgery may occasionally be required for patients to heal.
FAQs:
Is retrolisthesis a common condition?
Retrolisthesis is less common than its counterpart, anterolisthesis (forward displacement), but it can still occur. The prevalence and incidence of retrolisthesis vary depending on the population studied and the underlying causes.
Can retrolisthesis be hereditary?
There is no direct evidence to suggest that retrolisthesis is hereditary. However, certain congenital conditions affecting the spine can predispose individuals to develop retrolisthesis. It’s always advisable to consult with a healthcare professional for a proper evaluation if you suspect any spinal condition.Can retrolisthesis be treated without surgery?
Yes, in many cases, retrolisthesis can be managed without surgery. Non-surgical treatment options may include physical therapy, chiropractic care, pain management techniques, exercise programs, lifestyle modifications, and medications to relieve pain and inflammation.Is surgery ever necessary for retrolisthesis?
Surgery is typically considered when conservative treatments have failed to alleviate symptoms, or if the retrolisthesis is severe and causing neurological problems such as spinal cord compression or nerve root compression. The decision to proceed with the surgery is made on an individual basis, taking into account the patient’s specific condition.
How long does the recovery process take?
The recovery process for retrolisthesis can vary depending on the severity of the condition, the chosen treatment approach, and individual factors. In some cases, conservative treatment can lead to significant improvement within a few weeks to months. Surgical interventions may require a longer recovery period, typically ranging from several weeks to months before a return to normal activities.
Is retrolisthesis a permanent condition?
Retrolisthesis can be a chronic condition, but its progression and impact can vary among individuals. With appropriate treatment and management, including lifestyle modifications, physical therapy, and sometimes surgery, it is possible to alleviate symptoms and improve quality of life.