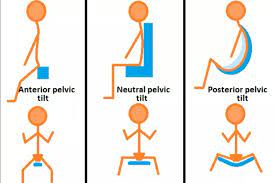
Difference between Anterior Pelvic Tilt and Posterior Pelvic Tilt
Anterior pelvic tilt and posterior pelvic tilt are two different postural deviations of the pelvis that can lead to various musculoskeletal issues and affect the overall alignment of the spine and lower body.
Table of Contents
What is Pelvic tilt?
Pelvic tilt (PT) is a position-dependent characteristic that is defined as the angle between the bifemoral heads’ centers and the vertical axis. The average anterior and posterior pelvic tilting ranges are 13.0 4.9° and 8.9 4.5°, respectively.
Pelvic Tilt Is Important (highlighted in green) – Anterior pelvic tilting exercises in the sagittal plane are commonly used to restore lumbar spine alignment in individuals suffering from persistent lower back pain (LBP). One of the primary causes of LBP has been recognized as a posture that supports lumbar lordosis. It is critical to limit the usage of the posture that causes lumbar lordosis while treating LBP.
Anterior pelvic tilting increases lumbar lordosis, whereas posterior pelvic tilting decreases it. Posterior pelvic tilting movements are frequently used in rehabilitation. The transversus abdominis is used in patients with excessive lumbar lordosis, whereas the multifidus is used in patients with diminished lumbar lordosis.
According to research, the local muscles are associated with anterior and posterior pelvic tilting and govern motion in the pelvic sagittal plane. Local muscle training may be useful for improving lumbar alignment in the sagittal plane in LBP patients. It may be beneficial to exercise the transversus abdominis in patients with excessive lumbar lordosis and the multifidus in those with diminished lumbar lordosis.
People with persistent low back pain have worse proprioception in the pelvic area, are less’ movement-aware,’ and may have poorer postural control. This raises the question of whether specific postures or activities that use extremes of certain motions (e.g., excessive or limited movement) may predispose persons to LBP.
“Pelvic tilt angle” is used to calculate anterior pelvic tilt. The angle formed by a line connecting the anterior superior iliac spines (ASIS) with a vertical line is commonly used to determine this measurement. The angle might be measured using a goniometer, with the patient lying supine on a table and the examiner palpating the ASIS to detect landmarks for measurement.
“Supine pelvic tilt test,” in which the patient is asked to lie supine with their knees bent and their feet flat on the table. The examiner then looks at the patient’s pelvic posture, noting any asymmetry or departure from neutral. Other investigations, such as the “prone hip extension test,” are applicable. It analyses posterior pelvic tilt and can suggest anterior pelvic tilt, and the “Thomas test,” which examines hip flexor tension and can indicate anterior pelvic tilt.
Recent studies have looked at the use of artificial intelligence (AI) in evaluating pelvic radiographs. Schwarz et al. (2023) employed a deep learning algorithm to examine over 500 pelvic radiographs in a research published in the journal International Orthopaedics and discovered that the AI software had an accuracy rate of over 90% in diagnosing fractures and other abnormalities in the pelvic area.
the adoption of AI-powered software might possibly increase the accuracy and efficiency of radiographic interpretation, especially when several pictures must be evaluated.
However, further study is required to assess the software’s efficacy in other clinical contexts and with various types of radiographs. This study demonstrates AI’s promise in medical imaging and its capacity to assist radiologists in their clinical practice.
Anterior Pelvic tilt
Anterior pelvic tilt (APT) is a frequent postural aberration characterized by excessive pelvic forward rotation. This posture has the potential to affect movement patterns, muscle imbalances, and injury risk.
APT is described as a forward tilt of the pelvis that results in increased lordosis of the lumbar spine and abdominal protrusion (Suits, 2021). It can be caused by a number of conditions, such as tight hip flexors, weak gluteal muscles, and bad posture. Some people may have a structural interpretation in their pelvis, like acetabular retroversion, which can contribute to APT.
A recent study has focused on the possible effects of APT on injury risk and sports performance. Mendiguchia et al. (2021) discovered that APT alterations were linked to hamstring strain injuries in football players. APT reduction with focused training interventions was specifically connected to a decreased risk of injury.
Brekke et al. (2022) studied the feasibility and advantages of exercise therapies for acetabular retroversion and excessive APT patients. They discovered that focused exercise programs improved symptoms and function, indicating that treating APT might have a favorable impact on people with this anatomical difference.
APT may be assessed using a number of clinical methods, including the pelvic tilt test and the Thomas test.
APT is frequently managed using stretching and strengthening exercises to correct musculoskeletal imbalances and improve posture. Individuals with structural differences may also require targeted therapies to optimize function and minimize symptoms.
Symptoms of Anterior Pelvic Tilt
Anterior Pelvic Tilt symptoms include frontal muscle tightness, low back discomfort, and improper posture. The most noticeable visual indication of Anterior Pelvic Tilt is an abnormal extension or curvature of the spine.
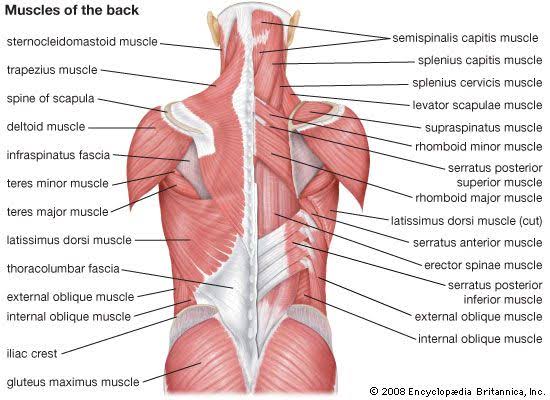
Muscles of the Anterior Pelvic Tilt
Anterior Pelvic Tilt is caused by many muscles. Anterior Pelvic Tilt is commonly caused by tight hip flexors and a weak core. The Psoas Major, Iliacus, Rectus Femoris, and Sartorius are the major hip flexors.
Posterior pelvic tilt
While posterior rotation is not uncommon in healthy people, it is significantly less common than normal pelvic angle. The alignment of the skeleton is also affected by a posteriorly rotated pelvis.
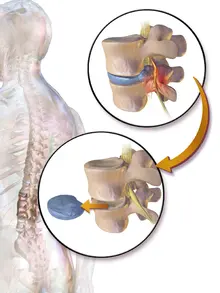
Turning the pelvis under flattens the lower back and reduces or eliminates the lower back curvature. Shearing forces propagate downhill through the lumbar spine without the lumbar curve, resulting in a pinching sensation at the top and bottom of the lumbar spinal segment.
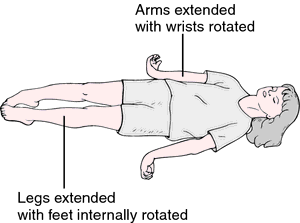
The hip sockets also reposition the femoral heads. The femur’s head and neck move horizontally rearward, resulting in an external (lateral) rotation of the leg. Whereas an anterior tilt leads the legs to spin inside, a posterior tilt causes the legs to rotate outward, resulting in the feet seeming to splay forth.
Pelvic Tilt Causes
Pelvic tilt can develop for a variety of reasons, and the causes can be fairly complex. The pelvis is affected by both cause and effect, which means that pelvic dysfunction can create other issues elsewhere, and other disorders can cause difficulties in the pelvis.
Worse, difficulties in the pelvis caused by other issues can exacerbate the original problem – a never-ending cycle of dysfunction causing pain, pain increasing dysfunction, and dysfunction increasing suffering and more pain.
Let’s start at the grounds and work up in glancing at the different causes and effects.
The Lower Body
- Rotation of the legs caused by one or both pronated or supinated feet might produce discomfort or soreness in the hip.
- To compensate, the pelvis tilts forward to reduce pressure on the hip joint.
- This tilt eventually causes low back pain and destabilization of the body’s core.
- Curves in the spine compensate, causing the head and neck to go forward.
- Leg length differences, which occur to some extent in the majority of the population, throw off hip leveling.
- The pelvis compensates by posteriorly sloping the short leg side of the pelvis.
- To maintain the eye level, a sideways strain occurs in the lower back, and a scoliotic “C” or “S” curve forms in the spine.
- Knee difficulties, habits, surgeries, muscle or nerve dysfunction, susceptibility (illness, heredity, structural deformity), and so on can all result in action at the knee.
- Most can cause knees to bend in or out of alignment with the appropriate angle between the upper and lower leg bones.
- When the legs bend inward (valgus knee), the pelvis rotates forward to compensate. Bowing out (varus knee) causes the pelvis to rotate backward.
The upper body
- Muscle laxity in the legs, hips, or abdomen destabilizes the body, causing the joints to adjust for instability. A succession of dysfunctions occurs, and crossing syndrome tilts the pelvis, freezes the hip joint, separates or jams the pelvic bones, and so on.
- Pregnantly carrying a child- The increased weight causes the tummy to protrude forward, the pelvis to twist anteriorly, and so on.
- Inadequate sitting or standing posture- This can work both ways: bad posture induces pelvic tilt, and pelvic tilt causes poor posture.
- Slouching causes the pelvis to rotate posteriorly, whereas sitting bolt upright causes the pelvis to move forward.
- Rounded shoulders and forward head posture certainly round the lower back and posteriorly rotate the pelvis.
- Rounding the shoulders with a ahead neck posture, but holding the low back from rounding, forces a person to anteriorly rotate their pelvis in order to compensate.
- Any number of hereditary predispositions and deteriorating diseases may cause excessive pelvic tilt.
Is Pelvic Tilt Correctable?
Manual treatment will prevent irreversible harm to musculoskeletal tissues by correcting functionally induced pelvic tilt.
Pelvic tilt can cause permanent injury to the ligaments, joints, disc material, and bones. While many of these develop naturally as we age, specialists have recently discovered degenerative diseases in younger groups. The sooner corrective action is sought and implemented, the quicker the cycle of pain and dysfunction may be broken. However, persistent vigilance must become the catchphrase. It’s all too simple to revert to bad posture habits, destroying all of your hard work.
What Is a Lateral Pelvic Tilt
Lateral Pelvic Tilt differs from anterior or posterior pelvic tilt in that it includes the pelvis sliding to one side (one hip being higher than the other). Hip drop or hip hike are other terms for lateral pelvic tilt. Muscular imbalances, poor posture/habits, differing leg limb lengths, or neurological disorders can all contribute to this.
Pelvic Tilt in sitting
Long durations of sitting might contribute to Anterior Pelvic Tilt. To fight this, it is advised that you break up your day and take some time to undertake Hip Flexor strengthening and stretching activities.
Pelvic Tilt Examination
- Your Physical Therapist can administer the Thomas Test to check for Anterior Pelvic Tilt.
- The hip flexors will be tested for flexibility in this test. You will lie on your back on a table with your legs dangling off the edge at the knees for this exam.
- Bring one knee up to the chest, holding underneath the knee.
- If the resting leg is no longer touching the table, the muscles in front of the thigh are probably quite tight, indicating a tilted pelvis.
- Your Physical Therapist can visually assess Posterior Pelvic Tilt.
- They may also ask you to squat to see whether you have a buttwink.
- Posterior Pelvic Tilt is indicated by a butt wink.
- Visual observation is usually sufficient to detect Lateral Pelvic Tilt.
- If one hand is higher than the other when both hands are placed on the top of the hips, this might suggest Lateral Pelvic Tilt.
Fixing Anterior Pelvic Tilt
- To correct Anterior Pelvic Tilt, you must first relax the hip flexors and promote hip flexibility.
- This is simply accomplished with everyday stretching.
- Try the half-kneeling hip flexor stretch, for example. In this stretch, you will assume a lunge stance with one knee touching the ground.
- Both of the knees should be at a 90-degree bend.
Fixing Posterior Pelvic Tilt
- Increase flexibility in the Hamstrings, Abdomen, and Glutes to correct Posterior Pelvic Tilt.
- Learn about dynamic stretches that will promote flexibility throughout the body by following exercises on how to execute a dynamic warm-up.
- To correct the Posterior Pelvic Tilt, you will also need to strengthen your hips and lower back.
Difference between anterior and posterior pelvic tilt
| Anterior pelvic tilt | posterior pelvic tilt | ||
| Definition | A forward tilt is called an anterior pelvic tilt. | A backward tilt is called a posterior pelvic tilt. | |
| Causes | -It is caused by the shortening of the hip flexor muscles. -The lengthening of the hip extensor muscles. -Extra belly weight, including pregnancy weight. -An anterior tilt can also result from extended sitting combined with inactivity. | -An imbalance between your leg muscles and core muscles, which include the pelvic floor muscles, transverse abdominis muscles, erector spine muscles, and diaphragm. – It is also caused by many of the same things as an anterior tilt. But, rather than flexing the back muscles, a person ends up slouching forward. -Bad sleeping posture | |
| Symptoms | -Low back pain -Tight pelvic and thigh muscles -A protruding belly -Possible knee, hip, and foot pain | -Low back pain -A slumped posture -Rolled-forward shoulders -Upper back tension -Tight hamstrings -Possible knee and hip pain | |
| Treatment and correctipon | -Do not sit for long periods, take regular breaks so that a person may stretch and walk. -Do not sit on the edge of the work chair, which tilts the pelvis forward even further. -Put a pillow or blanket between the knees to keep the pelvis in a neutral position while sleeping. Lose weight, if required. | -Make sure the desk height, chair height, and computer screen are all at the right level so that a person does not slump. -Get a chair with lumbar support, or put a smallish pillow behind the back while you sit. -Put a smallish rolled-up towel beneath the arch of the lower back as you sleep. -Wear a weight-training belt to keep the spine in a more neutral position. | |
| Exercises | -Squats -Lying pelvic tilt -Plank -Hip flexor stretches | -Abdominal press – ups(cobra pose) -Seated hamstring stretch -Glutes bridges -Straight leg raise -Back exercise( supermen exercise) |
Exercise to Correct Pelvic Tilt
Plank
To begin, place your elbows under your shoulders, your feet hip-width apart, and your toes tucked under.

- Squeeze your core and glutes and press up into a plank position.
- From head to shoulders, hips, knees, and ankles, your body should be in a straight line.
- Hold for 15-20 seconds, squeezing your core and glutes as hard as you can.
- Lower down slowly to rest for 10-15 seconds, then repeat 1-2 times more.
- Make sure the back doesn’t arch at the top of the bridge.
- You can plank on an elevated surface, like a bench or countertop, if planking on the floor feels too challenging.
Bridge with a band

- •Starting position: Put a medium resistance band just above the knees. Lay on the back with the knees bent, feet hip-width apart, and palms up as the arms rest at the sides.
- As a person elevate the hips, squeeze the glutes, and maintain tension on the band (keeping your knees hip-width and not allowing them to sink in).
- Raise your hips such that your shoulders, hips, and knees form a straight line.
- Squeeze the glutes as tight as possible while keeping the hips tucked under, then hold the highest position for 2 seconds before gently lowering down.
- Raise up into your next rep when your hips touch the ground.
- Avoid arching your back at the top of the bridge.
Hamstring curl with a ball
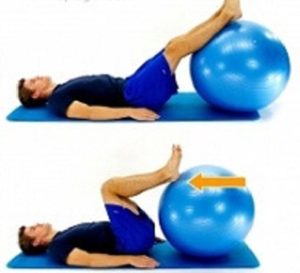
- •Lay on your back with your legs straight and your calves or ankles on top of the ball as your starting position.
- Rest your arms next to you to assist you with balance.
- The farther the ball is from your body, the more difficult the movement.
- Begin slowly, such as on the calves, and then move the ball aside to increase the difficulty as needed.
- As you elevate your hips towards the ceiling, squeeze your glutes and abs.
- As you roll the ball towards your glutes, keep your hips elevated and gently return to the beginning position.
- Note: If you find executing this exercise with your hips up too difficult, try it with your hips down.
- Begin with your legs straight, pressing your heels into the ball as you roll it towards you in a flowing manner. The hamstrings should still be active.
For optimal results, repeat your pelvic tilt program 2-4 times per week and/or before each workout. After a few weeks of constant stretching and strengthening, you should see a reduction in any pelvic tilt-related lower back discomfort.
Summary
In summary, the main difference between anterior pelvic tilt and posterior pelvic tilt is the direction in which the pelvis tilts. APT involves a forward tilt of the pelvis and an excessive arch in the lower back, while PPT involves a backward tilt of the pelvis and a flatter lower back.
Both conditions can have adverse effects on posture and can lead to discomfort and pain if left unaddressed. It’s important to maintain proper pelvic alignment and address muscle imbalances through exercises and postural awareness to prevent or correct these issues.
FAQ
What exactly is the distinction between anterior and posterior pelvic tilt?
While anterior pelvic tilt is caused by the front of the pelvis moving forward and the rear of the pelvis rotating upward, posterior pelvic tilt is caused by the front tilting up and back and the bottom rotating beneath the body.
Which of the following pelvic tilts is the most common?
Both of these rotations can result in low back and hip discomfort, as well as poor posture, biomechanics, and gait patterns. An anterior pelvic tilt (more frequent in women) has a forward rotation. Consider your pelvis to be a bucket, and you are dumping water in front of you. In other words, your pelvis is forward-tilted.
What are the causes of anterior and posterior pelvic tilt?
This issue occurs when your hip flexor muscles shorten after sitting for an extended amount of time. These tense muscles force the pelvis forward, causing it to tilt anteriorly. Pelvic tilt to the back. This condition occurs when your hip extensors shorten, causing your pelvis to tilt back.
Do women have an anterior pelvic tilt?
Anterior pelvic tilt is a postural alteration caused by the front of the pelvis rotating forward and the rear of the pelvis rising. According to some studies, up to 85 percent of males and 75 percent of women with no symptoms have an anterior pelvic tilt.
Yoga can help with anterior pelvic tilt.?
Ekhart Yoga offers yoga for anterior pelvic tilt.
There are several yoga positions and stretches that target the hip flexors, such as lunges and warrior poses. We can also use balancing activities to shift the pelvic bones into a more neutral position rather than leaning forward.
References
Pelvic tilt. (n.d.). Physiopedia. https://www.physio-pedia.com/Pelvic_Tilt
& S. Z. K. (2023). The difference between an anterior and posterior pelvic tilt. Your House Fitness. https://www.yourhousefitness.com/blog/the-difference-between-an-anterior-pelvic-tilt-and-posterior-pelvic-tilt
Pelvic tilt –. (2017, May 25). https://www.mbmyoskeletal.com/learning/pelvic-tilt/
Mahaffey, K. (n.d.). Posterior & anterior pelvic tilt: How do you fix it? https://blog.nasm.org/what-is-pelvic-tilt-how-do-you-fix-it