Bennett Fracture
Table of Contents
What is a Bennett Fracture?
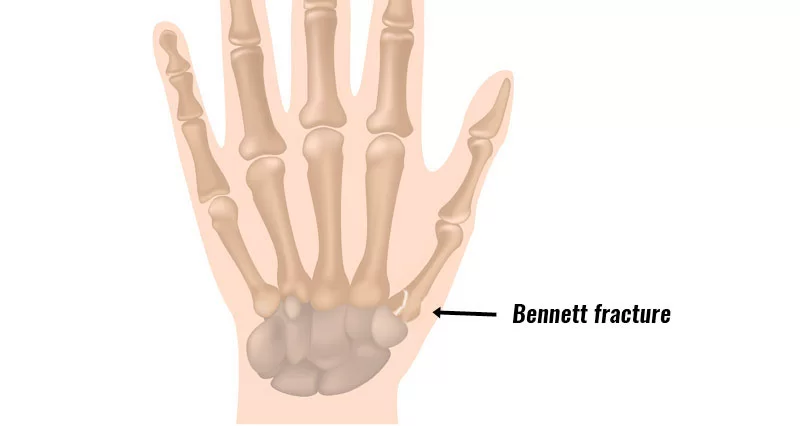
A Bennett fracture is a specific type of fracture that occurs at the base of the thumb, affecting the joint called the first carpometacarpal joint. This joint connects the thumb metacarpal bone (the bone in the palm of the hand that connects to the thumb) to the wrist.
A Bennett fracture typically happens when a force is applied to the thumb in a specific manner, such as during a fall or direct impact. The fracture involves the articular surface of the first metacarpal bone, which means that the joint surface is disrupted.
Definition
A Bennett fracture takes place when the first metacarpal gets pushed into an abducted position, fracturing the base of the thumb. It is described as an intra-articular two-part fracture of the base of the 1st metacarpal bone.
- Despite a fairly simple appearance on radiographs, Bennett’s fractures are believed not stable.
- In assessing and treating these fractures placing the patient with a thumb extension position also known as the hitchhiker position must be prevented as this will result in additional fracture displacement.
- If there is a sufficient alignment of the fracture pieces at postsurgical fixation, clinical results are typically adequate.
- She was called later Edward Hallaran Bennett (1837-1907), a famous surgeon from Dublin, Ireland.
Clinically Anatomy and Pathophysiology
The isolated articulation of the first CMCJ is found between the trapezium and the base of the first metacarpal, resulting in an extremely uncommon joint.
- The articulation is saddle-formed which permits multidirectional movement.
- ligaments in this joint are the anterior (volar) and posterior (dorsal) oblique ligaments, the volar and dorsal intermetacarpal ligaments, and the posterior radial ligament.
- The volar oblique ligament is the most necessary for stability in the carpometacarpal joint.
The fracture type is different.
- The base of the first metacarpal is fractured with an intraarticular extension because the palmar ulnar fragment of the 1st metacarpal is maintained in position by its ligamentous join to the trapezium (volar oblique ligament) during the axial loading with the rest of the metacarpal moving in the opposite direction and the primary fracture line happening along with this moment of weakness.
- Because of this fracture, the first metacarpal shaft subluxated posteriorly, proximally, and radially because of the pull of the abductor pollicis longus, extensor pollicis longus, extensor pollicis brevis, and the adductor pollicus brevis, which stay connected to the fracture segment.
Common Causes of Bennett’s Fractures
Bennet fractures happen when the thumb experiences sufficient force for it to flex, damage, and dislocate. Athletes, for example, boxers, football or rugby players, and martial artists, are more prone to Bennett’s fracture because of how frequently they experience direct contact with a flexed thumb. While such sports frequently result in breaks, falls and accidents can also result in Bennet’s fracture.
Symptoms and signs of Bennett Fracture
Symptoms of Bennett fracture are instability of the CMC joint of the thumb, attended by the presence of pain and pinch grasp weakness. Expected symptoms include discomfort, ecchymosis, and swelling close to the thumb’s base and thenar eminence, especially over the thumb’s CMC joint.
Physical examination reveals that the thumb’s CMC joint is unstable. Typically, the patient will show weakness when trying to hold objects or do actions like tying shoes or tearing paper. Other complaints contain extreme pain undergone upon catching the thumb on an object, for example when going into a pants pocket.
Mechanism of injury
The Bennett fracture is a diagonal intraarticular metacarpal fracture dislocation, resulting from an axial force directed in front of the partially flexed metacarpal. This kind of reduction across the metacarpal bone is usually maintained when a person hits a hard thing, for example, the skull or tibia of an opponent, or a wall. It can also happen as a consequence of a fall onto the thumb. This is a typical injury supported by bike falls, as the thumb is typically extended while near the handlebars. It is also a typical trauma in car crashes, particularly in fixed things, from the driver maintaining the steering wheel during impact. The hand pushes forward, while the steering wheel rim hyperextends the thumb.
Differential Diagnosis
Rolando fractures, extra-articular fractures, and the gamekeeper’s thumb are further predicted injuries to the first metacarpal.
The 1st differentiation indication can be seen during the examination or palpation of the area of the damage. The existence of edema and ecchymosis on the carpal metacarpal joint of the thumb, as well as complaints of pain and weakness in the pinch grip, are all indications of a Bennett fracture. The individual will be not able to complete functional tasks for example attempting a shoe or utilizing a key. Likely complications may be an infection, malunion or un-union, arthritis, and stiffness with contracture.
Examination
If a Bennett fracture is questioned, the patient’s personal history must include an injury to the hand or thumb that was evident by immediate pain, edema, or ischemia. The most familiar cause of the trauma is an axial impact (compression) involved in the thumb whilst in flexion.
During physical assessment, Bennett’s fracture of the 1st carpometacarpal joint may exist with:
- observable deformity in case of the fracture is displaced
- complain of pain and swelling +/- ecchymosis on the carpo metacarpal joint of the thumb
- tenderness to palpation
- elevated temperature around the place in the acute phase
- reduced pinch grasp and reduced strength of the grip
Although X-ray films may be utilized to analyze this situation, a CT scan must be ordered to assess the length of the damage. A Bennett fracture may show up on these CT scans as an intra-articular fracture and a dislocation of the base of the first metacarpal. Even though there is a dislocation there must still be a slight fragment of the 1st metacarpal that persists to articulate with the trapezium.
Medical Treatment of Bennett Fracture
In stable, undamaged fractures, non-operative treatment in a thumb spica cast for three to four weeks can be evaluated.
Surgical treatment is suggested for not stable fracture type and intra-articular displacement of more than 1 mm. While open reduction and internal fixation with a screw or K-wire are both standard methods, screws are frequently chosen as K-wires must be released after the union.
The treatment algorithm is also affected by the age and occupation or hobbies of the patient.
Untreated or malunion fractures can result in secondary osteoarthritis. Osteoarthritis or malunion can result in significant pain and functional decline.
Physical Therapy Treatment
Normally, hand fractures are managed by immobilization with a cast or splint however of whether operative or conservative management was needed.
Physiotherapists and occupational therapists are commonly greatly involved in developing and adjusting these in consultation with the treating group or surgeon.
- Protocols for rehabilitation must be dep[end on the stability of the fracture and fracture management (operative or nonoperative).
- Following the immobilization period, physiotherapists and specialist hand therapists are involved in the facilitation of restoring maximal performance to the hand.
- The range of motion exercises can start 5 to 10 days after-screw fixation and later four weeks after pinning (after the pins are dismissed).
- Modalities used possess cryotherapy, mobilization of the joint, strengthening & flexibility exercises, dexterity re-education, and specific instruction.
- Exercise intensity and complexity must be advanced properly next to the selected protocol commonly provided by the surgeon.
- Many reports show that initial physiotherapy treatment promotes function and return to work or sport in hand fractures.
Complications of Bennett Fracture
The capacity to grasp, pinch, and resist the thumb is essential for a number of daily tasks. In actuality, the thumb does about 50 percent of the entire hand function. An intact and working thumb CMC joint is necessary for these abilities. The CMC joint of the thumb permits a broad range of movement while keeping stability for grasp and pinch.
In accordance with this, lacking correctly identifying and treating the Bennett fracture will result in a hand with barely complete function in addition to an unstable, painful, and arthritic CMC joint with a restricted range of movement.
The volar oblique ligament, which is connected to the tubercle of the trapezium bone of the CMC joint, holds the proximal metacarpal fragment in place in the case of the Bennett fracture. This ligamentous attachment confirms that the proximal fragment stays in its proper anatomical position.
The distal fragment of the first metacarpal bone keeps the majority of the articular surface of the first CMC joint. Strong hand ligaments and muscle tendons, in contrast to the proximal fracture segment, have a tendency to draw this fragment out of its ideal anatomical place of residence.
Especially:
- tension from the abductor pollicis longus muscle (APL) subluxations the piece in a posterior, radial, and proximal direction
- tension from the APL turns the piece into supination
- tension from the muscle adductor pollicis (ADP) displaces the metacarpal head into the palm
Even when the fracture segments are initially in their proper anatomic position, tension from the muscles APL and ADP continuously causes the fracture fragments to shift. Bennett fractures almost always require some sort of treatment due to the aforementioned biomechanical traits in order to guarantee healing in the correct anatomical position and restoration of the thumb CMC joint’s proper function.
Prognosis
If intraarticular trapeziometacarpal fractures (for example the Bennett or Rolando fractures) are permitted to recover in a displaced position, important after-traumatic osteoarthritis of the base of the thumb is almost assured. Some form of operative treatment (commonly either a CRPP or an ORIF) is almost constantly suggested to secure an adequate result for these fractures if there is significant displacement.
The long-term result after operative treatment appears to be identical, whether the CRPP or the ORIF procedure is utilized. Especially, the general strength of the involved hand is typically diminished, and after-traumatic osteoarthritis tends to evolve in nearly all circumstances. The degree of weakness and the severity of osteoarthritis does yet appear to correlate with the quality of reduction of the fracture. Therefore, whether by the CRPP or the ORIF operation, the goal of treating Bennett fractures should be to accomplish the greatest reduction possible.
Conclusion
The treatment of Bennet’s fracture is complicated and sufficiently done with an interprofessional team that possesses a hand surgeon or orthopedic surgeon, thing care nurse, and a physiotherapist.
When the fracture is experienced by the emergency department doctor and nurse practitioner, it is necessary to refer the patient promptly to a hand surgeon.
Inadequately managed bennet fracture has very great morbidity. Even after satisfactory treatment, extensive rehabilitation is required.
The consequences of Bennet fracture are guarded
FAQ
A clean fracture with a significant bone fragment missing is caused by a Bennett fracture, which occurs at the base of the thumb metacarpal in relation to the CMC joint. A Rolando fracture is identical to a Bennett fracture, besides that rather than a clean crack, the bone is broken into many pieces.
Symptoms of Bennett fracture are instability of the CMC joint of the thumb, attended by present pain, and pinch grasp weakness. Typical signs contain pain, swelling, and ecchymosis near the base of the thumb and thenar eminence, particularly on the CMC joint of the thumb.
For Bennett fractures with a trapeziometacarpal joint displacement of between one and three millimeters, closed reduction and percutaneous pin fixation (CRPP) using K-wires is typically sufficient to produce a satisfactory functional result.
Diagnosis can be caused by orthogonal radiographs of the thumb. For certain extra-articular fractures, treatment options range from splint immobilization to surgical fixation for displaced Bennett or Rolando fractures. The majority of Bennett and Rolando’s fractures were caused by axial stress being applied to the thumb in flexion.
Athletes will have a complaint of pain and swelling mentioned at the base of the thumb. Active movement is limited due to pain. Once proper suspicion of a fracture is present, traditional posteroanterior, lateral, and oblique radiographs (x-rays) must be accepted.
Introduction Bennett’s trauma is a fracture subluxation of the 1st carpometacarpal joint. The causative mode is axial excess across the first metacarpal with coexisting flexion. The palmar oblique ligament keeps the palmar marginal component in its anatomical situation.
A clean fracture with a significant bone fragment missing is caused by a Bennett fracture, which occurs at the base of the thumb metacarpal in relation to the CMC joint. A Rolando fracture is identical to a Bennett fracture, besides that rather than a clean crack, the bone is broken into many pieces.
Symptoms of Bennett fracture are instability of the CMC joint of the thumb, attended by present pain, and pinch grasp weakness. Typical signs contain pain, swelling, and ecchymosis near the base of the thumb and thenar eminence, particularly on the CMC joint of the thumb.
For Bennett fractures with a trapeziometacarpal joint displacement of between one and three millimeters, closed reduction and percutaneous pin fixation (CRPP) using K-wires is typically sufficient to produce a satisfactory functional result.