Adductor canal syndrome
Table of Contents
What is Adductor canal syndrome?
- Adductor canal syndrome (also known as adductor canal compression syndrome) is the rare, non-atherosclerotic cause of arterial occlusion & limb ischemia. There is the compression of the superficial femoral artery (SFA) in the adductor canal.
- Sports such as running, skiing && soccer are at risk for the development of this rare entity. It should be noteworthy that female involvement with reference to adductor’s canal syndrome is infrequent. Palma substantiated this observation by arguing that female patients display a more oblique femur position & a larger adductor canal.
Anatomy
- The adductor canal (subsartorial, & Hunter canal) is an aponeurotic tunnel in the middle third of the thigh, enlarging from the apex of the femoral triangle to the opening in the adductor Magnus, the adductor hiatus.
- It is 15 cm long & serves as a passageway for structures moving between the anterior thigh & posterior leg.
Structure
Boundaries of the adductor canal.
- The Adductor canal is bordered by muscular structures:
- Anterior: Sartorius.
- Lateral: Vastus medialis.
- Posterior: Adductor Longus & adductor magnus muscle.
- The apex of the adductor canal is marked by the adductor hiatus – a gap between the adductor & hamstring attachments of the adductor Magnus.
- It is covered by a strong aponeurosis, the anteromedial intermuscular septum (subsartorial fascia) which extends from the vastus medialis, across the femoral vessels to the Adductor Longus & adductor Magnus. Lying on the aponeurosis is the sartorius muscle.
Content
- The canal contains the following:
- Femoral artery
- Femoral vein
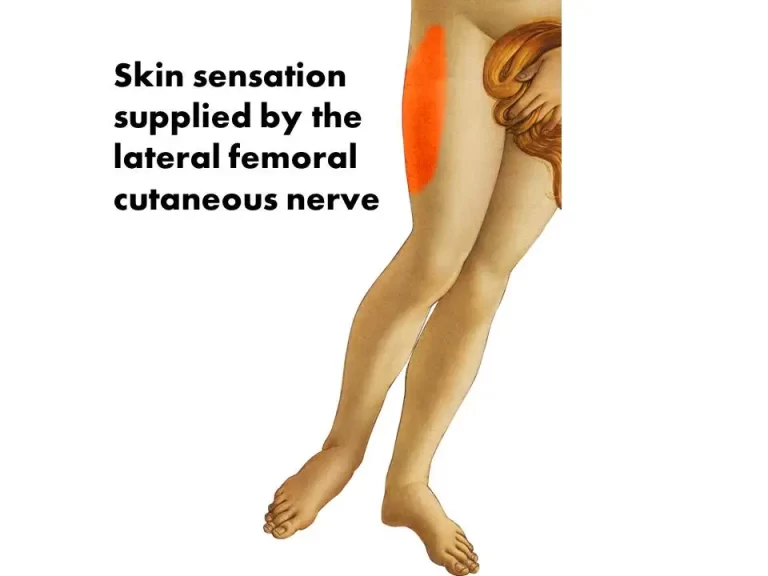
- Branches of the femoral nerve (specifically, the saphenous nerve, & the nerve to the vastus medialis).
Adductor Canal is represented in the green region.
It consists of 3 foramina: superior, anterior, & inferior.
- The femoral artery with its vein & the saphenous nerve enters this canal through the superior foramen. Then, the saphenous nerve & artery & vein of genus descendants exit through the anterior foramen, piercing the vastoadductor intermuscular septum. Finally, the femoral artery & vein exit via the inferior foramen (usually called the hiatus) through the inferior space between the oblique & medial heads of the adductor Magnus.
Epidemiology
- External compression of the superficial femoral artery in the absence of atherosclerotic risk factors causing adductor canal syndrome is rare & available data is limited to case reports. The syndrome is most generally reported in young males less than 45 years old.
Clinical Symptoms of Adductor canal syndrome
- The symptoms can differ depending on the occlusion. They present with symptoms of acute limb ischemia. Compression of the saphenous nerve without vascular collusion causes pain over the medial portion of the knee. Symptoms involved:
- exercise-induced claudication
- paraesthesia
- pain
- edema (due to femoral vein compression)
- pallor
- poikilothermia
- thrombosis leading to acute limb ischemia
Pathology
- There is chronic external compression of the superficial femoral artery as It route through the adductor canal. This results in harm to the vessel, in situ thrombosis, limb ischemia, & potential limb loss. The arise of external compression may begin from either an anomalous musculotendinous band arising from the adductor Magnus & hypertrophy of the adductor Magnus or vastus medialis muscles.
Diagnosis
- Usually, athletes suffering from hunter canal syndrome complain about exercise-induced calf pain & paresthesia. In particular, numbness of the toes seems to be a pertinent symptom. Concerning neurological differential diagnosis, the sports medicine physician may further keep in mind saphenous nerve entrapment at the adductor canal which could become symptomatic as anterior knee pain.
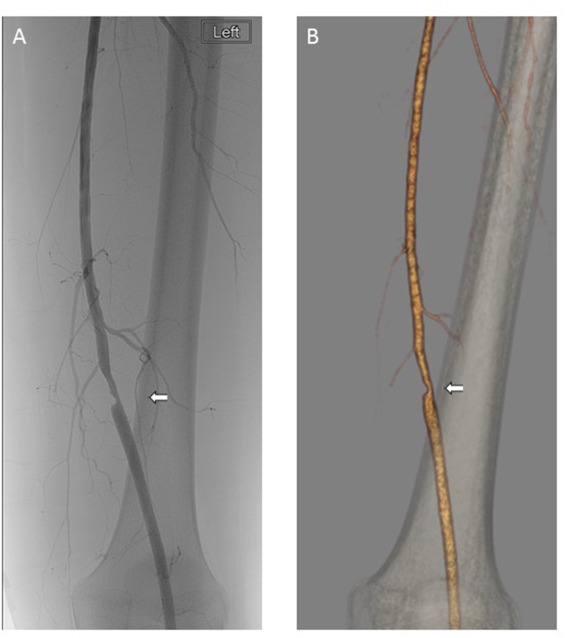
- In case of pain at rest & pulselessness also thrombotic vessel occlusion has to be taken into thought. Accordingly, exercise ABPI studies, duplex ultrasonography, & angiography should be of assistance in establishing the diagnosis. Surrounding soft tissue may be asses by MRI.
Differential diagnosis
- popliteal artery entrapment syndrome
Treatment & prognosis of Adductor canal syndrome
- Treatment is always surgical & involves resection or release of the external compressive forces. Angioplasty or bypass of the diseased superficial femoral artery may be needed if the mechanical compression has caused vascular damage.
- Acute limb ischemia due to thrombosis from hunter canal syndrome needs immediate revascularisation either via endovascular thrombolysis or thromboembolectomy. Diagnosis of adductor canal syndrome might prompt investigation for the same condition on the contralateral side.
- Surgical treatment of adductor’s canal syndrome is unavoidable. Hence, resection of unusual musculotendinous bands plus vein patch angioplasty (or bypass of the destructed artery segment) constitutes standard care in these patients. According to Ehsan et al. short-term results are good & most athletes are capable to return to previous performances. Regrettably, long-term data are still scarce.