
Abductor Pollicis Longus Muscle
Table of Contents
Description
The abductor pollicis longus muscle is a muscle located in the forearm, on the lateral side of the forearm. It is one of the muscles responsible for the movement of the thumb, specifically for abducting (moving away from the hand) and extending the thumb.
The abductor pollicis longus muscle originates from the posterior surface of the ulna bone and the interosseous membrane in the forearm. It then inserts into the base of the distal phalanx of the thumb.
This muscle is innervated by the posterior interosseous nerve, which is a branch of the radial nerve. It receives its blood supply from the posterior interosseous artery.
Injuries to the abductor pollicis longus muscle can occur due to overuse or trauma and can result in weakness or inability to perform certain thumb movements. Rehabilitation exercises and physical therapy may be necessary to recover from such injuries.
Origin of Abductor pollicis longus muscle
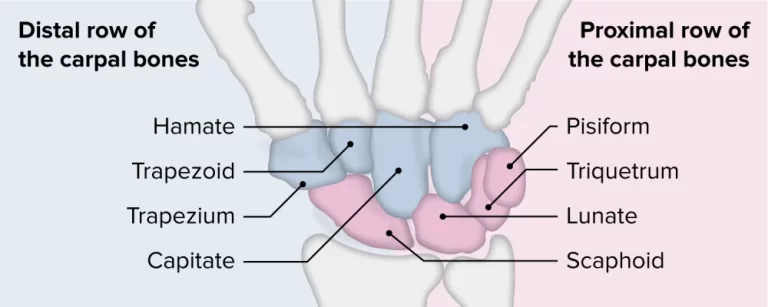
It originates from the hand’s flexor retinaculum, the scaphoid bone’s tubercle, and sometimes from the trapezium’s tubercle as well.
Insertion
It is inserted into the capsule of the metacarpophalangeal merged as a thin, flat tendon on the little finger side of the base of the 1st phalanx of the thumb.
Relations
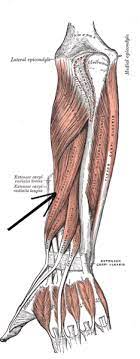
- The abductor pollicis longus muscle belly is situated on the posterior side of the forearm’s distal half.
- Its tendon is outside the tendon of the extensor pollicis brevis, and it is situated deep to the extensor digitorum and laterally to the extensor pollicis longus muscle.
- The superficial part of the abductor pollicis longus is traversed by the posterior interosseous nerve and artery, which goes in the middle of the extensor digitorum and abductor pollicis longus.
- The outermost border of the anatomical snuffbox is created by the tendon of the abductor pollicis longus.
- The styloid process of the radius is located distally and the posterior compartment of this triangular space is at the base of the thumb.
- The neurovascular construction of the hand traverse the anatomical snuffbox; the cephalic vein, the radial artery, and the superficial branch of the radial nerve.
- The extensor pollicis longus (medial) and brevis (lateral) bones are absolute at this space’s borders, while the scaphoid and trapezium bones are from the floor.
Innervation
The posterior interosseous nerve (C7, C8), which prolongs the deep radial nerve, innervates the abductor pollicis longus. A division of the posterior cord of the brachial plexus is the radial nerve.
Blood supply
- The interosseous branches of the ulnar artery give the abductor pollicis longus muscle blood;
- The lateral branch of the posterior interosseous artery provides the muscle’s proximal portion.
- The distal part is modified by a puncturing part of the anterior interosseous corridor.
The function of the APL muscle
- The function of the abductor pollicis longus muscle is to stretch the thumb aside from the palm either on its own or in co-occurrence with the abductor pollicis brevis.
- More specifically, at the 1st metacarpophalangeal joint, it causes (mid-) extension and abduction of the thumb.
- This activity is found in exercises such as bowling and scooping.
- The muscle also assists the thumb in fully extending at the metacarpophalangeal joint, working with the long and short extensors.
- When letting go of priorly held objects, for example, this movement is important for releasing the hand grip.
- Furthermore, the abductor pollicis longus assists in the radial deviation of the hand at the radiocarpal joint.
Clinical Relevance
- DeQuervain’s Syndrome is the most crucial clinical condition that affects the APL, generally in co-occurrence with the Extensor pollicis brevis.
- The 1st extensor compartment of the wrist feels pain and swelling as an outcome of thickening and inflammation of the APL and EPB tendons.
- The tendons are more susceptible to degeneration and lesions due to pain are worse when the thumb is working.
Assessment of Abductor Pollicis Longus Muscle
- The subject is suggested to abduct the thumb at that time holding the forearm in a neutral position to calculate the strength of APL.
- In the direction of the thumb’s adduction, force is applied against the lateral aspect of the 1st metacarpal’s distal end.
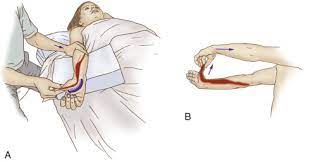
- Finklestein’s test is the one that was utilized to make a clinical diagnosis for DeQuervains.
- The patient is asked to form a 1st by inserting the thumb in the middle of the digits.
- The therapist or examiner moves the wrist to the little finger’s side.
- Pain over the radial styloid process at the part of the APL and EPB tendons is a sign of a positive test.
Abductor pollicis longus muscle stretching
- To perform a stretch of the Abductor pollicis longus muscle, start with performing adduction and flexion of the thumb at the carpometacarpal joint, and radial deviation of the hand at the wrist joint.
Abductor pollicis longus muscle strengthening exercise
Thumb isometrics
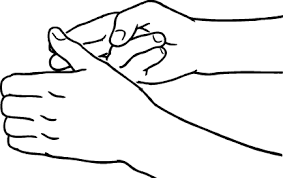
- The thumb muscles may be reinforced in various headings with this activity.
- Try to make a fist with the thumb and use the other hand to give pressure in both directions to get initiative.
- To resist the pressure, hold for 10 seconds with an upright thumb.
FAQ
Ice can reduce pain and swelling. Experts recommend doing it for 10 to 20 minutes every 2 to 3 hours for 3 to 5 days, or until the pain is gone. Compress the area using an elastic bandage or tape. Take anti-inflammatory painkillers.
Any overuse muscle pain or injury to the abductor pollicis longus may happen because of hand or wrist sprains, leads to pain with stiffness mainly wrist and thumb movements. Another relevant cause for pain in the abductor pollicis longus is De Quervain’s tenosynovitis, a condition generally provoked by continuous strain or overuse of the wrist and thumb.
Rest and save the involved area or sore groin area for 1 to 2 weeks. Stop, change, or take a break from any activity that can be causing pain or soreness. Do not perform intense activities while you still have pain.
If the tear is high on the adductor tendon, recovery may be notably slower and take approximately 12-16 weeks. A tear to the mid-belly of the muscle will typically take in the middle of 4 and 12 weeks to heal depending on the severity of the tear.
One Comment