Wrist Dislocation
Table of Contents
What is a Wrist Dislocation?
Wrist dislocation occurs when the bones of the wrist are forced out of their normal positions. It is usually caused by a sudden impact or a fall onto an outstretched hand. Wrist dislocations can vary in severity, ranging from a partial dislocation where the bones are partially displaced to a complete dislocation where the bones are completely out of place.
The most common type of wrist dislocation is a complete dislocation, where the bones in the wrist completely separate from each other.
Introduction
- Wrist dislocations can occur at the radiocarpal joint, the midcarpal joint, and the distal radioulnar joint or may describe a variety of these injuries in painful trauma. Carpal instability in the need of the lunate and peri semicircular dislocations are unstable injuries that can live usually be failed. Distal radioulnar joint dislocations are most typically associated with distal third radius ruptures. This injury complex is named a Galeazzi fracture-dislocation.
- Intrinsic ligaments hold the carpal bones together, whereas extrinsic ligaments connect the carpus to the radio- and ulnocarpal joints. Disorder of these ligaments results in wrist instability. The prevalence of carpal instability is centered on the lunate, given its place in the midpoint of the wrist. Injuries move sequentially relying on the rigor, from scapholunate instability to lunate dislocation.
- Perilunate dislocations and lunate dislocations are elevated wrist injuries affecting motor vehicle collisions or muscular injuries. While not familiar, these injuries can result in a group of complications. Despite the incredible force typically needed, up to 25% of these injuries are forgotten clinically and radiographically. Perilunate and lunate dislocations with an associated rupture are twice as dominant as those without rupture.
Anatomy
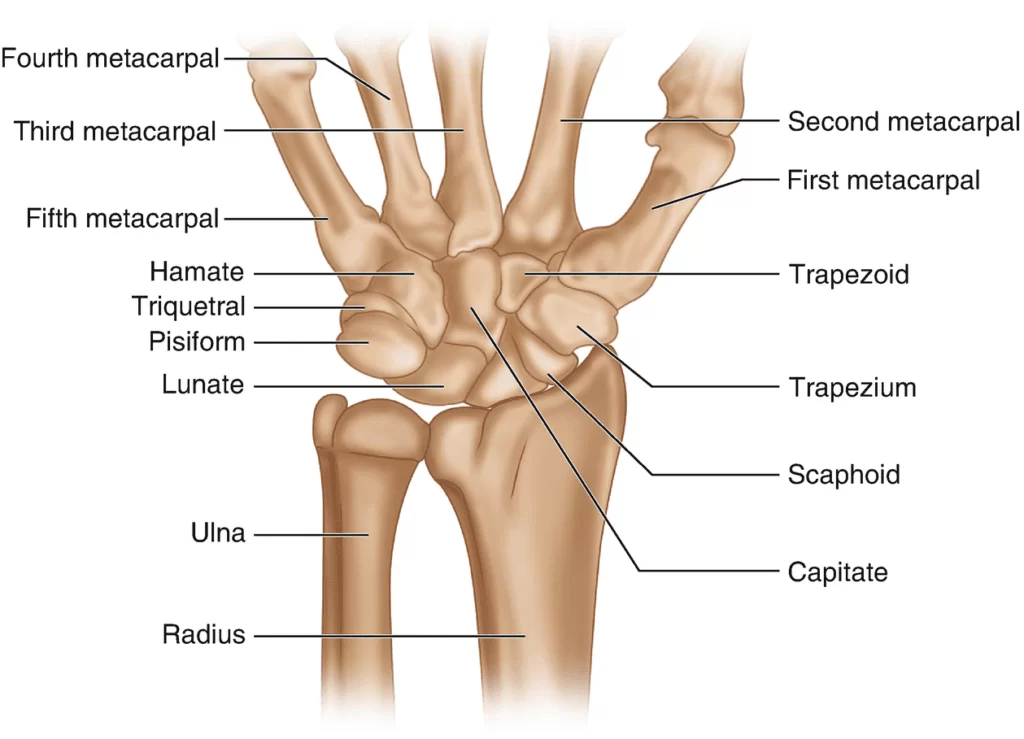
The wrist joint, also known as the radiocarpal joint, is a complex joint that allows for a wide range of movements. It is formed by the articulation of several bones, ligaments, and tendons.
- Non-essential ligaments maintain the carpus’s associations to the metacarpals distally and the radius and ulna in tight. The intrinsic ligaments connect the carpal bones individually further.
- The volar extrinsic ligaments are more muscular resembling the dorsal extrinsic. The quick radio lunate ligament is a volar ligament joining the lunate to the distal radius.
- While a dislocated wrist can affect all eight carpals, your lunate and scaphoid bones stand usually involved.
- These two bones create a bridge between the radius and ulna bones in your forearm and the further, fewer bones in your wrist.
The Distal Radioulnar Joint
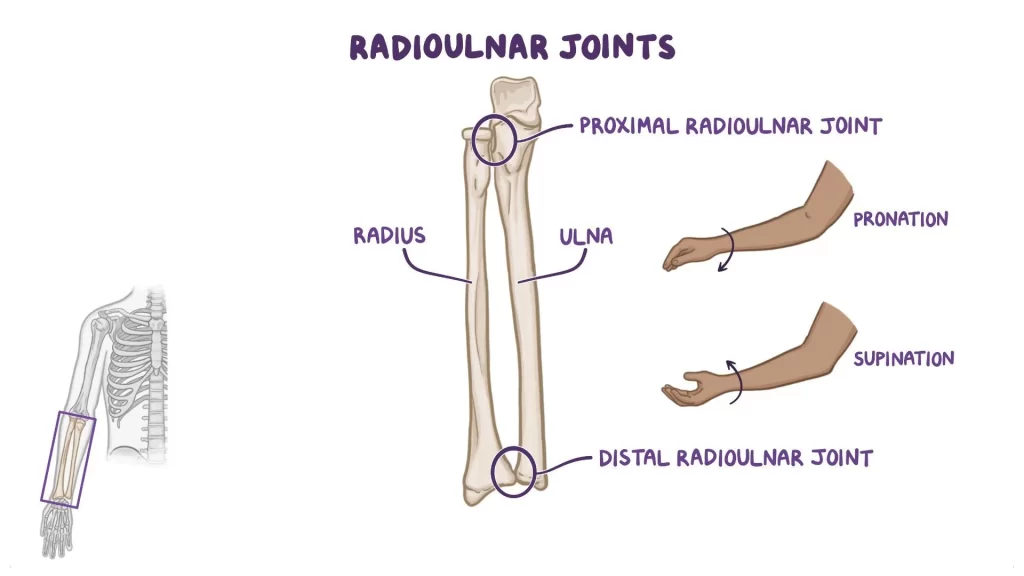
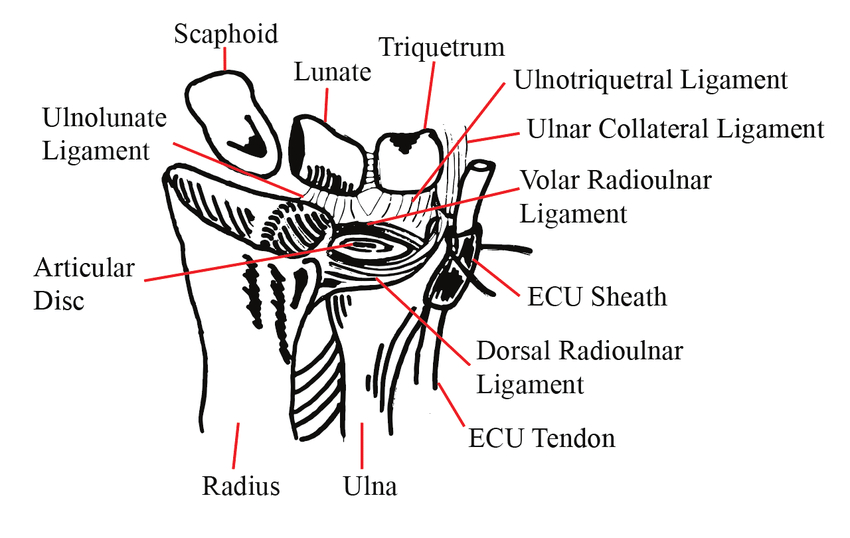
- The distal radioulnar joint is mainly stabilized by the deep dorsal and volar radioulnar ligaments within the fovea of the triangular fibrocartilage complex (TFCC).
- The lunate is a crescent-shaped carpal bone that communicates with the distal radius proximally, and the capitate distally. It is found between the scaphoid radially and the triquetrum clearly in the proximal row of carpal bones. The scapholunate, capitulate, and lunotriquetral intrinsic ligaments all stabilize the position of the lunate in the wrist.
- There are no firm tendinous insertions onto the lunate. The proximal carpal row is partially irregular when reached by the distal forearm and distal carpal row, resulting in a more elevated tendency for injury.
- Carpal instability is often the effect of concussion. These injuries often result in a drop on an outstretched hand, during which an axial significance is required on the carpals with the wrist in hyperextension.
- Injury moves about the lunate in a semicircular way depending on the severity of the injury.
- The Mayfield type affects 4 stages describing the sequence of ligamentous and carpal disruptions caused by wrist hyperextension, ulnar deviation, and intercarpal supination reliably reproduced on cadavers.
- The scapholunate ligament is disrupted in the rather phase, resulting in flux between the scaphoid and lunate. In the two-phase, there is a disorder of the yield accent resulting in likely dislocation of the capitate.
- In the third phase, there is a disorder of the lunotriquetral declaration resulting in the lunate dislocating dorsally.
- In the fourth and last phase, there is a loss of the dorsal radiocarpal ligament, and this affects the volar dislocation of the lunate into the carpal tunnel.
Epidemiology:
- Wrist fracture dislocations are typical. Sheltered dislocations are irregular.
Types Of Dislocated Wrist
Many varieties of dislocated wrists, but mainly Four types of dislocated wrists.
- Anterior lunate dislocation. The lunate bone rotates while the further wrist bones remain in position.
- Perilunate dislocation. This classification affects the lunate bone and the three ligaments around it.
- Galeazzi fracture. This classification applies to a rupture in your radius bone and dislocation of your radioulnar joint.
- Monteggia fracture. This applies to a rupture in your ulna and dislocation of one of the ends of your radius.
Most wrist dislocations affect either an anterior semicircular dislocation or a peri-lunate dislocation.
Symptoms
A dislocated wrist is mostly characterized by aching discomfort that is significantly exacerbated when you try to move your wrist up and down or side to side. Your forearm also suffers from your strength.
You may even see the following about your wrist:
- Bruising
- Deformity
- Extreme and immediate pain
- Inability to use joint or limb normally
- Numbness
- Redness
- Weakness
- swelling
- Tenderness
- Discoloration or bruising. If your lunate bone is affected, it may push against the nerves in your wrist. This can provoke tingling or numbness in your fingers.
Causes
Any type of traumatic impairment to your hand or arm can result in a dislocated wrist. Typical reasons for these injuries contain:
- High-impact classifications, such as football or hockey
- Car accidents
- Breaking a slip with your hand
- In increase, the pressure on the ligaments in your wrist can result in a dislocated wrist.
- This grade of stress tills to arrive from accomplishing something that set a constant strain on your wrist, such as walking with crutches.
Diagnosis
- To prevent the injury from becoming worse, make an immediate conversation with your doctor as soon as you consider a wrist injury.
- Your doctor will begin by adjusting your wrist in various positions before asking you whether you experience any discomfort.
- They can use this information to identify the ligaments and bones that may be affected. The nerves, blood vessels, and tendons that feed the hand and wrist will be examined by your doctor to see whether any harm was done.
- To confirm a diagnosis, they’ll probably take an X-ray of your hand and forearm next.
- An MRI may be used by your doctor to assist them define a diagnosis if it appears you have a ligament that has ruptured. This imaging test provides more explanation.
Simple radiographs - To detect a wrist displacement, an x-ray sequence of the wrist that includes AP, lateral, and oblique views is required.
- Despite the fact that carpal instability injuries are commonly overlooked, the diagnosis should be possible by utilizing these straightforward videos.
Lines from gilula
Gilula described the following three lines on an AP of the wrist:
- The scaphoid, lunate, and triquetrum of the proximal carpal row.
- The proximal carpal row’s distal end
- The capitate and hamate’s proximal aspect

- When Gilula’s lines are disrupted on the AP view, the physician should be highly suspicious of a potentially dangerous injury.
- The distance between the ulnar border of the wrist’s radial
- Less than 3 millimeters separate the radial border of the lunate from the ulnar border of the scaphoid in typical wrist radiographs. Posteroanterior radiographs may show an enlarged scapholunate space, sometimes known as the “Terry Thomas” sign, in cases with scapholunate dissociation.
- Obtaining a grip compression view can replicate the anomalous gap detected if the damage is not visible on standard wrist films. The scaphoid rotates to a more transverse position when scapholunate ligament instability takes place.
- As a result, the scapholunate angle increases to more than 60 degrees. The “signet-ring sign” occurs when the scaphoid shortens and forms a thick ring-like image around its distal edge.
- The lunate will be correctly aligned with the distal radius in cases with perilunate dislocations, while the capitate will be dorsally displaced. A perilunate dislocation might minimize scaphoid and lunate carpal bone fractures that are present.
- The lunate is shown displaced volar on the lateral x-ray in lunate dislocations, while the distal radius, carpus, and metacarpals are otherwise aligned normally.
- This symbol is also known as the “spilled teacup” sign. Due to the lunate’s rotation in a volar direction, a lunate dislocation will seem distinctively triangular from the posteroanterior perspective.
- “The “piece of the pie sign” is what is used to describe this.
Treatment
Medical and surgical care
- A technique known as a reduction is typically used to cure mild dislocations. Your doctor carefully moves the bones back into place during this operation. Depending on the extent of your injuries, this may be pretty painful. Your doctor will first provide either local or general anesthesia to lessen the discomfort.
- You’ll likely need to wear a splint or cast after the treatment to keep your wrist from moving while it heals. A sling can also be required of you.
- Surgery may be required to straighten your wrist bones or to mend damaged ligaments in more severe situations. Securing everything in place is occasionally done using pins or screws.
Physiotherapy rehabilitation
- Five to ten minutes of ice cubes or a cold pack
- Hot pack
- Rehab exercises
- Rest
- Electrotherapy
Exercises for treating wrist fractures:
- The goal is to increase wrist muscle strength and flexibility in order to reclaim pain-free mobility.
- Unless otherwise specified, the duration is 4–6 weeks.
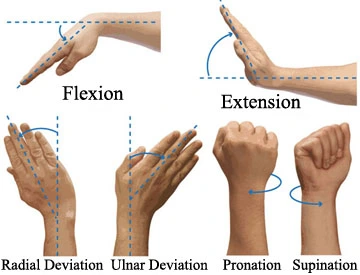
- Range of motion at the wrist
- Wrist stretch: Pressing the back of your hand down and holding it there for 15 to 20 seconds with one hand can assist bend the opposite wrist downward.A minute, Perform this workout 3 times.
- In order to extend the hand back, push the fingers backward and hold that position for 15 to 30 seconds. Maintain a straight elbow during this exercise. Perform this workout 3 times. Tip: Maintain a straight elbow during this workout.

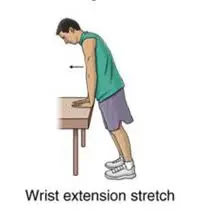
- Wrist Extension Stretch: Stand at a table with your elbows straight, palms down, and fingers flat. Your entire body should lean forward. Maintain this position for 15 seconds.
3 Repetition.
- Wrist Flexion Stretch: While standing with your elbows straight and your palms up and your fingers facing inward, place the backs of your hands on a table.
For 15 seconds, maintain this posture.
3 Repetition.
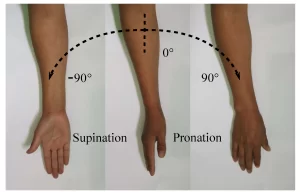
- Pronation and supination of the forearm: Hold your arm out to the side with your elbow bent 90 degrees. palm upward, then hold for five seconds.
Move your palm slowly downward and hold for five seconds.
Throughout this exercise, maintain your elbow at your side and bent 90 degrees.
Do three sets of ten.
Tip: Once this exercise is pain-free, try performing it while holding something heavy in your hand, such as a soup can or hammer handle.
- Exercises for Strengthening: 6, 7, and 8.
- Wrist Flexion: Place your palm down and hold a hammer or soup can handle in your hand. Bend your wrist upward gradually.
Put the weight at the beginning position while gradually lowering it.
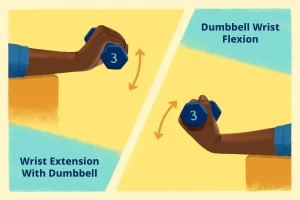
- Wrist Extension: Hold a hammer can handle in your hand, palm down. Bend your wrist upward gradually. Put the weight at the beginning position while gradually lowering it.
Do three sets of ten.
Hint: Increase the weight of the item you’re holding gradually.To strengthen your grip, squeeze a rubber ball (like a stress ball) and hold the position for five seconds.Do three sets of ten.
Prognosis
- The prognosis is based on a variety of variables.
- One can anticipate a reasonable outcome if a patient’s wrist dislocation is discovered and treated quickly.
- There is a larger chance of developing post-traumatic arthritis in the presence of recurring instability and aberrant carpal biomechanics.
- Scapholunate progressive collapse may develop in patients with persistent scapholunate dissociation.
Complications
- The most typical reason for wrist degenerative arthritis is scapholunate dissociation. The capitate may migrate closer to the scaphoid and lunate if it is not identified and treated right away.
- Scapholunate advanced collapse, often known as the SLAC wrist, is the outcome of this degenerative condition.
- A frequent long-term consequence after perilunate and lunate injuries is wrist osteoarthritis.
- Avascular necrosis of the lunate, chronic carpal instability, tendon ruptures, delayed union, nonunion, and malunion, as well as compression of the median nerve, are additional problems.
FAQ
Bones, ligaments, tendons, and nerves can all suffer harm when the wrist dislocates. You could require more care. Your wrist was placed back in its proper place by the doctor, who may have also given it a cast or splint. Your wrist will remain steady up until your follow-up goes because of this.
Avascular necrosis of the lunate, chronic carpal instability, tendon ruptures, delayed union, nonunion, and malunion, as well as compression of the median nerve, are additional problems.
Bones, ligaments, tendons, and nerves can all suffer harm when the wrist dislocates. You could require more care. Your wrist was placed back in its proper place by the doctor, who may have also given it a cast or splint. Your wrist will remain steady up until your follow-up visit thanks to this
The most typical kind of wrist dislocation is perilunate dislocation. The scaphoid, triquetrum, and other carpal bones around the lunate are displaced dorsally, but the lunate itself is still in its usual position with regard to the distal radius.
Your arm may be kept raised and supported using cushions or pillows, which will also improve your comfort. You must place it higher than your heart. It is usual for discomfort to be worse at night, but this should pass within the first two weeks if you take some medications before bed.
It is known as a Galeazzi fracture-dislocation injury complex. The incidence of radiocarpal dislocations in wrist injuries ranges from 0.2% to 2.7%. About 7% to 10% of all reported injuries to the carpal bones are caused by carpal instability.
Severe discomfort, visible wrist deformity, and tingling in the thumb, index, and middle fingers are all symptoms. It’s critical to get early medical assistance from a trained hand and wrist expert for a potential dislocated wrist due to the complexities of the wrist joint.
The capitate and lunate are the two bones of the hand and wrist that are most frequently injured in dislocations. The biggest bone in the hand, the capitate, is situated in the lower palm. The lunate is a long bone in the forearm that lies between the capitate and the ulna.
The lunate dislocation, perilunate dislocation, and scapholunate dissociation are the three wrist dislocation forms that occur most frequently.
When the radius, one of the two long bones in the forearm, fractures at the wrist, it is said to have a distal radius fracture. Fractures of the distal radius occur often. In actuality, the radius is the arm bone that breaks the most frequently.