
What is Decerebrate rigidity? Cause, Symptoms, Diagnosis, Treatment
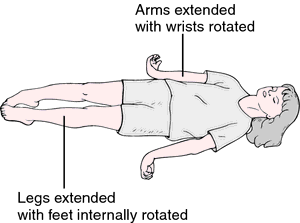
Decerebrate rigidity is a type of abnormal posture in which Body is in extendser rigid body position – the arms and legs are in extended rigid straight out, the toes being pointed downward, and the head and neck being arched backward. The muscles are in rigid that body is in extended. This type of abnormal posture usually means there has been severe damage to the brain.
Decerebrate rigidity is also called decerebrate response, Decerebrate posture or extensor posturing.
In this position the involuntary extension of the upper limb in response to external stimuli. In decerebrate rigidity, the head is hyperextended back, the arms are also extended by the sides, and the legs are extended.
Decerebrate rigidity is caused by damage to the cerebral cortex but the clinical symptoms varies depend on the site of the lesion. Causes of decerebrate rigidity are seizures,tumors, vascular lesions, and trauma. Spontaneous nystagmus or eye deviation is also seen in decerebrate rigidity. This type of rigid posture usually shows that there has been severe damage to the brain.
In Decerebrate rigidity is a rare type of posture seen in people who have injuries to their brainstem and is a rarely seen medical condition, in which the body position- upper extremities are held outstretched and internally rotated. In this position, the arms are pronated with the forearms held vertically, the toes being pointed downward, and the head and neck being arched backward. The legs are also extended and pronated.The patient is rigid, with the teeth clenched. This kind of rigid posture seen mostly in severe midbrain lesions.
Decerebrate rigid posture can occur on one side or both sides, or in just the arms or limbs. It is also associated with another type of abnormal posture called decorticate posture. A person who have decorticate posture on one side of the body while at the opposite side decerebrate rigid posture in few severe cases.
Opisthotonos may occur in severe cases of decerebrate rigid posture where a severe muscle rigidity of the neck and back are seen. The Nobel Laurette Charles Sherrington first time described decerebrate rigidity posture in 1898 after transecting the brainstems of live monkeys and cats.
Decerebrate rigid posture are considered pathological rigid responses to usually unpleasant stimuli from an external or internal, in which stereotypical extended body movements of the trunk and limb are seen.
Table of Contents
Which are the Causes of Decerebrate rigidity?
Following are the few most common Causes of decerebrate rigid posture are
- Haemorrhage in the brain from any cause
- Brain tumour
- Brain Abscess
- Hemorrhagic Stroke
- Brain affected mainly due to side effect of drugs, poisoning or fungal , Bacterial infection
- Head- brain injury
- Brain injury due to liver failure
- Increased pressure in the brain from any cause such as Hydrocephalus
- Low blood sugar (hypoglycaemia)
- Brain tumour
- Infections, such as meningitis
- Intracerebral hemorrhage.
- Reye syndrome ( liver function and brain damage related problems that mostly affects children)
- Brain injury from lack of oxygen
- Cerebral malaria
- Lead poisoning
In patients with all-ready have severe Brain-damage, episodes of decerebrate rigidity can occur in response to numerous unpleasant external or internal stimuli such as fever, hypoxia; metabolic disturbance; sensory irritation; hypoglycemia; and meningeal irritation.
Symptoms of Decerebrate rigidity:
Following are the most common symptoms of decerebrate rigid posture, however it may vary depends upon lesion and type of Injury :
A severe muscle spasticity or rigidity of the neck and back may occur in severe cases of decerebrate rigid posture also called Opisthotonos posture.
In Decerebrate rigidity, movement pattern are adduction and internal rotation of the shoulder, extension at the elbows with pronation of the forearm, and flexion of the fingers and the lower limbs movement pattern are Hip extended and internally rotated with the knee also extended and Ankle are plantar flexed while Toes are typically abducted and hyperextended.
The patient is in rigid state with the teeth clenched.
The decerebrate rigid posture can be seen on just one side of the body or on both sides, and it may be only in the arms and may be both arms and legs in severe trauma.
In severe Trauma A person can also have decerebrate rigidity on one side of the body while at the opposite side decorticate posture can be seen.
Glasgow Coma Scale (for adults) is nearly about 2 score a patient displaying decerebrate rigidity in response to pain (Motor section) and Pediatric Glasgow Coma Scale (for infants), due to his or her muscles extending because of the neuro-muscular response to the stimuli (external or internal).
A person with decorticate posturing may gradually start to show decerebrate rigidity, or may go from one form of posturing to the another.
Progression from decorticate posturing to decerebrate rigidity is mostly indicats that transtentorial or tonsilar brain herniation.
Decerebrate rigidity responses to usually unpleasant stimuli from an external or internal where exetends arms and leg movements of the trunk and extremities are typically indicative of significant brain or spinal cord injury.
Diagnosis :
Following are the method are most commonly used to Diagnosis of Decerebrate rigidity.
- A computerized tomography scan (CT Scan)
- Magnetic Resonance Imaging- of Head (MRI)
- Blood and urine tests to examine blood counts, screen for drugs and toxic substances, and measure body chemicals and minerals
- Cerebral angiography (dye and x-ray study of blood vessels in the brain)
- EEG (brain wave testing)
- Intracranial pressure (ICP) monitoring
Prognosis:
Study shows that Patients have head injury with decerebrate rigidity have surviving ration nearly about 10%.
Children with head injury with decerebrate rigid posture are admitted to Hospital in ICU have have a mortality of 10% to 13%; however, in severe cases the mortality ratio is nearly 71%.
Different scientific studies have also shown similar mortality rates of 68% to 83% in TBI with decerebrate rigidity.
Normally people showing decerebrate or decorticate rigidity are in a coma and have poor prognoses, with risks for cardiac arrhythmia or arrest and respiratory failure.
Factors that involved positively in survival in TBI with decerebrate rigid posture are younger patient age, admission within as early as possible hours of injury, and extradural hematoma. Negative factors are mostly acute subdural hematoma and older age.
Treatment of Decerebrate rigidity:
Emergency ICU Treatment (Mostly Neauro. NICU).
Emergency Craniotomy for evacuation of extra-axial hematoma can improve survival.
Remove the cause (Treatment depends upon Diagnosis and symptomatic) eg. correcting if possible metabolic derangements or / and treating infections.
Symptomatic supportive treatment are started.
Physiotherapy treatment in Decerebrate Rigidity:
Physiotherapy treatment and exercises are used to treat and improve the symptoms of decerebrate rigid posture. The most common treatment for decerebrate rigidity is postural rehabilitation, which uses exercises and physiotherapy treatments to improve the muscles that support the spine and to improve the posture of the spine.
Postural exercises are used to improve the posture of the spine and to strengthen the muscles that help support the spine. Decerebrate rigidity is often treated with a series of exercises that are designed to improve the posture of the spine, strengthen the muscles that support the spine, and stretch the muscles that are tight due to the position of the head and shoulders.
Following are the most commonly follow treatment are used , However it vary depends upon symptoms, causes and Diagnosis of the condition.
- Relax Passive Movement
- Chest Physiotherapy
- Reduce rigidity / spasticity
- Regular Stretching exercise
- Rehabilitation Program
- Postural correction
- Regular Ankle Movement
- Stretching exercise
- Regular change the position if patient is in coma stage (Mostly supine to side lying position to avoid Bed sore)
Range of Motion exercise :
Passive relax passive range of motion (ROM) exercise helps to avoid joint stiffness and deformities. One a daily passive movement of all four limb and trunk are required.
Stretching exercise:
To reduce spasticity / rigidity regular Stretching exercise are the best treatment option.
Stretching exercise of tight muscles mainly Hamstring, calf and adductors muscles stretching exercise are important in lower limb and relax passive movement to maintain range of motion are also equally important.
In Upper limb according to assessment of spasticity/rigidity stretching exercise are started. Maintain Range of Motion with the help of relaxed passive movement of all joint is beneficial.
To improve Balance of Sitting Balance and standing Balance, according to assessment Balance exercise are started for overall rehabilitation to improve condition.
Strengthening exercise in Decerebraate rigidity:
Strengthening exercise of weak muscles according MMT (Manual muscle testing) are started , that will help overall posture correction and Rehabilitation. All four limb and trunk muscle strengthening exercise are also depends upon assessment.
Posture correction:
Orthosis / Splint are also use to correct deformities and posture.
Decerebrate rigidity damage to what part of brain ?
Following Brain area are damaged in the Decerebrate rigidity:
large bilateral forebrain lesions with progression caudally into the diencephalon and midbrain.
posterior fossa lesion compressing the midbrain or rostral pons.
the level between the superior and inferior colliculi within the midbrain (being at or below the level of the red nucleus)
Latest studies shown that the vestibulospinal tract plays a major role in decerebrate posturing. The vestibulospinal pathways have an excitatory effect on extensor motor neurons in the spine, while inhibition of flexor motor neurons.
The vestibular nuclei receive input from the vestibular apparatus and spinal somatosensory pathways while receiving modulatory signals from the cerebral cortex and the fastigial nucleus of the cerebellum.
The vestibular nucleus, via the vestibulospinal tract, causes activation of extensor motor neurons in the spinal cord and inhibition of flexor motor neurons. However, under normal physiology, the higher brain centers of the cortex and cerebellum inhibit the vestibular nuclei, thus preventing this reflex. Decerebrate posturing results from a disconnection between the modulatory higher centers and the vestibular nuclei, resulting in unsuppressed extensor posturing.



Thank you. Very helpful having the word for this now.