
True vs Apparent Leg Length
Table of Contents
Introduction:
True leg length and apparent leg length are terms used to describe differences in leg length, which can have various implications for an individual’s posture, gait, and overall health. True leg length refers to the actual anatomical length of the bones in the legs, measured from the hip joint to the ankle joint. Apparent leg length, on the other hand, is the perceived difference in leg length due to factors such as pelvic tilt, scoliosis, or other structural imbalances that affect the alignment of the pelvis and spine.
Leg length difference (LLD) in the lengths of a patient’s lower limbs are usually described as leg length discrepancies. Obliquity of the pelvis is typically caused by abnormalities in limb length.
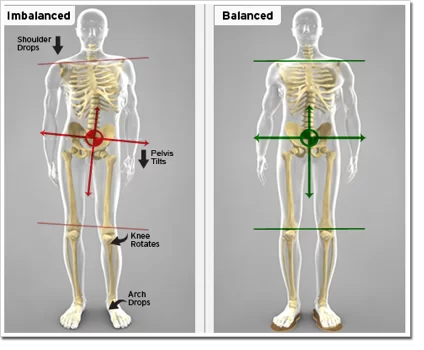
Pelvic inversion When a patient is standing normally, the two sides of the pelvis should be level with one another. The patient is instructed to stand with their backs to the examiner in order to assess for pelvic obliquity. The patient should be barefoot, with their feet together and their knees completely extended. After that, the examiner inserts one or two fingers from each hand on the patient’s iliac crests. Imagines drawing a line between the two crests after that. Pelvic obliquity exists when this fictional line is not perpendicular to the ground.
Anisomelia, also known as leg length discrepancy (LLD), is a disorder in which the paired lower extremity limbs are markedly different in length. Leg length difference (LLD) has long been a contentious topic among academics and medical professionals. Although its existence is acknowledged, there is little agreement regarding its many aspects, such as the degree of LLD deemed to be clinically significant, the prevalence, validity, and reliability of the measuring techniques, the impact of LLD on function, and its significance in a number of neuromusculoskeletal conditions.
TYPES: There are numerous potential causes of obliquity, but they may be generally categorized into two categories: those that create a functional, or apparent leg length discrepancy and those that induce a true leg length discrepancy.
Leg lengths are described as true and apparent in terms of their absolute and adjusted lengths. To determine if there is any leg length discrepancy, the limb length measurement is used.
The body adjusts for limb shortening by lowering the pelvis, placing the foot in an equinus posture, and flexing the opposing lower limb at the hip and knee.
What is True and Apparent Leg Length?
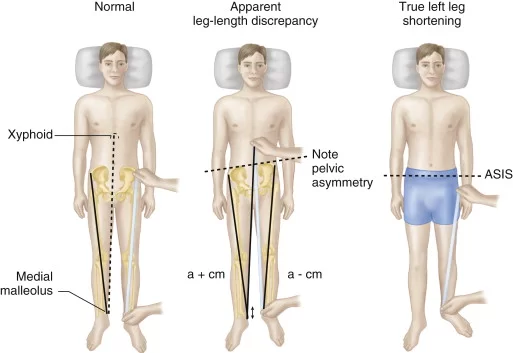
When both lower limbs are in the same postures and the pelvis is square, the length is measured from the anterior superior iliac spine to the tip of the medial malleolus. Please take note that the lower reference point ASIS [anterior superior iliac spine] is outside the limb, and any variation in position might alter the length, making the same position of the lower limb and pelvic squaring extremely essential.
The lack of a reference point forces us to use the anterosuperior iliac spine, a convenient reference point, even though the correct length of the limb should be measured from the middle of the femur to the medial malleolus.
Similar to true length, apparent length is measured with the following exceptions:
There is an unsquared pelvis.
The limbs are not placed in the same location.
The umbilicus and xiphisternum serve as the common upper reference points.
In essence, the deformity is left alone, and the length of the limbs is measured from a common location, such as the umbilicus or xiphisternum.
Both limbs are measured independently, and the difference between the readings is computed to determine the apparent and genuine shortening. The difference in the perceived lengths of two limbs is known as apparent shortening.
The difference between two genuine lengths is referred to as true shortening.
The term “appearance of shortening” refers to the impact of deformity on the actual shortening.
If the genuine shortening is the same as the perceived shortening, no compensation has occurred.
The real shortening is more than the apparent one, a portion of the shortening has likely been made up for.
If there is a fixed adduction deformity in addition to the apparent shortening and no compensation, then the genuine shortening is smaller than the apparent shortening.
True Leg Length:
- True leg length refers to the actual anatomical length of the bones in the lower limbs, from the hip to the ankle.
- It is measured from a fixed point on the pelvis, usually the anterior superior iliac spine (ASIS), to a specific landmark on the lower limb, often the medial malleolus of the ankle.
- The measurement is taken in a straight line along the axis of the bones, and it reflects the skeletal structure of the individual.
- True leg length provides a direct assessment of bone length and can be valuable for evaluating conditions such as leg length discrepancies, where one leg is shorter than the other due to differences in bone growth or developmental factors.
Apparent Leg Length:
- Apparent leg length refers to the perceived difference in leg length due to various factors, including pelvic tilt, spinal curvature, and postural changes.
- It is measured similarly to true leg length, from a fixed point on the pelvis to the medial malleolus. However, due to postural abnormalities, the measurement may not accurately represent the actual bone length.
- If the pelvis is tilted or the spine has curvature, such as in cases of scoliosis, the apparent leg length on one side may appear shorter or longer than the true leg length. This is because the altered alignment affects the relative position of the pelvis and spine.
- Apparent leg length differences can result from issues unrelated to bone length itself, such as pelvic rotations, lumbar lordosis (swayback), or other postural adaptations.
True Versus Apparent Leg Length Discrepancy:
True leg length discrepancy and apparent leg length discrepancy are two distinct concepts used to describe differences in leg length. These discrepancies can have different causes and implications. Here’s a comparison between true and apparent leg length discrepancies:
True Leg Length Discrepancy (LLD):
Definition:
True leg length discrepancy refers to the actual difference in anatomical bone length between the two lower limbs. It is a measurable and quantifiable variation in the length of the bones in the legs, typically measured from a fixed point on the pelvis (such as the anterior superior iliac spine) to a specific anatomical landmark on the ankle (such as the medial malleolus).
True LLD can result from factors such as unequal bone growth, congenital conditions, fractures, or surgical procedures affecting bone length. This type of discrepancy can have significant implications for biomechanics, gait patterns, joint function, and overall musculoskeletal health.
Causes of True Leg Length Discrepancy (LLD):
- Unequal Bone Growth: Differences in the rate of bone growth during childhood and adolescence can lead to true LLD. This can be influenced by genetic factors or conditions that affect bone development.
- Congenital Conditions: Certain congenital conditions, such as congenital hip dislocation or developmental dysplasia of the hip, can result in asymmetrical bone growth and true LLD.
- Fractures: Fractures that occur in the bones of the legs during growth can lead to discrepancies in bone length during the healing process.
- Surgical Procedures: Surgical interventions involving bones, such as orthopedic surgeries or joint replacements, can sometimes result in LLD if the alignment is not perfectly restored.
- Bone Conditions: Bone disorders, such as osteomyelitis (bone infection) or osteochondroma (bone tumor), can affect bone growth and potentially lead to true LLD.
Symptoms of True Leg Length Discrepancy (LLD):
- Gait Abnormalities: People with true LLD may develop an altered walking pattern to compensate for the discrepancy. This can include a limp, uneven steps, or favoring one leg over the other.
- Muscle Imbalances: A significant true LLD can lead to muscle imbalances in the hips, pelvis, and lower back. This can result in overuse of certain muscles and weakness in others, leading to discomfort or pain.
- Back Pain: Uneven leg lengths can contribute to poor posture and increased stress on the spine. This may lead to lower back pain, especially in the lumbar region.
- Hip Pain: The altered mechanics caused by true LLD can affect hip joint alignment and function, leading to hip pain or discomfort.
- Knee Pain: Uneven leg lengths can also impact the alignment and function of the knee joint, potentially leading to knee pain or issues such as patellofemoral syndrome.
- Ankle and Foot Problems: True LLD can influence the mechanics of the ankle and foot, potentially leading to issues like overpronation, plantar fasciitis, or Achilles tendon problems.
- Uneven Shoe Wear: Individuals with true LLD may notice uneven wear on their shoes, with one side of the sole wearing down more quickly than the other.
- Functional Limitations: Depending on the severity of the discrepancy, individuals may experience limitations in daily activities, sports, or exercise due to altered biomechanics.
- Joint Stress: The joint stress resulting from compensatory movements can lead to degenerative changes over time, increasing the risk of conditions like osteoarthritis.
- Postural Changes: True LLD can contribute to postural changes, with one shoulder appearing higher or one hip being more prominent than the other.
- Muscle Fatigue: Compensating for the difference in leg lengths can cause certain muscles to work harder than normal, leading to muscle fatigue and discomfort.
Measurement of True Leg Length Discrepancy (True LLD):
True leg length refers to the actual anatomical length of the bones in the lower limbs, measured from a fixed point on the pelvis to a specific anatomical landmark on the lower limb. This measurement is essential for assessing leg length discrepancies and guiding treatment decisions. Here’s a detailed explanation of true leg length and the measurement procedure:
Anatomical Landmarks:
- The measurement of true leg length involves two primary anatomical landmarks:
- Anterior Superior Iliac Spine (ASIS): The ASIS is a bony projection located on the front and upper portion of the pelvis. It’s commonly used as the starting point for measuring true leg length.
- Medial Malleolus: The medial malleolus is the bony prominence on the inner side of the ankle. It’s located on the tibia bone and serves as the endpoint for measuring true leg length.
Measurement Procedure:
- Patient Positioning:
- The patient should lie down on an examination table in a supine (lying on the back) position.
- The legs should be extended fully and parallel to each other.

2. Locating the ASIS:
- The examiner identifies the ASIS on both sides by palpating the bony projection at the front of the pelvis, just above the hip joint.
- The ASIS is marked on both sides using a skin marker or a removable adhesive marker.
3. Identifying the Medial Malleolus:
- The examiner identifies the medial malleolus, which is the bony prominence on the inner ankle, specifically on the tibia bone.
4. Measurement:
- A measuring tape or caliper is used to measure the distance between the marked ASIS and the identified medial malleolus on both sides.
5. Recording the Measurements:
- The measurement for each leg is recorded separately.
- The measurement is typically recorded in centimeters (cm) or inches (in).
6. Calculating the Difference:
- The difference between the measurements of the two legs indicates the leg length discrepancy.
- A positive difference indicates that one leg is longer than the other, while a negative difference indicates that one leg is shorter.
Clinical Considerations:
- True leg length measurements provide a direct assessment of the bone length and are not influenced by postural changes or alignment issues.
- Leg length discrepancies are common and can be due to various factors, including congenital conditions, growth discrepancies, or acquired conditions.
- The degree of leg length discrepancy and its potential impact on gait and biomechanics will determine the need for intervention, such as orthotics, lifts, or surgical procedures.
Accuracy of Measuring True Leg Length Discrepancy (True LLD):
- High Accuracy: True leg length discrepancy measurement tends to be highly accurate, as it involves directly measuring the actual bone length from fixed anatomical landmarks (ASIS to medial malleolus).
- Less Influence by Postural Factors: True LLD measurements are less influenced by postural changes, pelvic tilt, or spinal curvature because they directly assess bone lengths.
- Precision: Measurements taken using proper tools and techniques by trained professionals are typically precise and reproducible.
Factors Affecting Accuracy:
- Examiner Skill: The accuracy of both types of measurements is influenced by the examiner’s experience and skill in identifying landmarks and using appropriate measurement tools.
- Patient Positioning: Accurate patient positioning is crucial for obtaining reliable measurements in both true and apparent LLD assessments.
- Patient Variability: Anatomical variations among individuals can impact accuracy. For example, variations in the prominence of bony landmarks can affect measurement accuracy.
Clinical Considerations:
- To ensure the highest accuracy, measurements should be taken by qualified healthcare professionals using standardized protocols and appropriate tools.
- For true LLD, accuracy is generally higher due to the direct measurement of bone lengths.
- For apparent LLD, accuracy is influenced by the examiner’s ability to account for postural changes and identify landmarks consistently.
Assessment of True Leg Length Discrepancy (True LLD):
- History and Examination:
- Obtain the patient’s medical history, including any history of fractures, surgeries, or congenital conditions that may have affected bone growth.
- Perform a physical examination to identify any asymmetry in bone landmarks, joint positions, or gait patterns.
2. Measurement:
- Measure the true leg length by assessing the distance between the anterior superior iliac spine (ASIS) and the medial malleolus on each leg.
- Calculate the difference between the measurements to determine the true LLD.
3. Imaging:
- If necessary, imaging studies such as X-rays may be ordered to assess the bone length and alignment, as well as identify any structural abnormalities.
4. Clinical Considerations:
- Assess the impact of the true LLD on gait mechanics, joint function, and musculoskeletal health.
- Determine whether the LLD is causing symptoms such as pain, discomfort, or biomechanical issues.
5. Treatment Planning:
- Based on the severity of the discrepancy and its impact, healthcare professionals may recommend interventions such as orthotics, lifts, physical therapy, or surgical procedures.
Management of True Leg Length Discrepancy (True LLD):
- Orthotic Devices and Shoe Lifts:
- For mild to moderate true LLD, custom-made shoe lifts or orthotic devices can be used to equalize leg lengths and improve alignment.
2. Physical Therapy:
- Physical therapy focuses on addressing muscle imbalances, joint stiffness, and gait abnormalities associated with true LLD.
- Targeted exercises aim to improve muscle strength, flexibility, and coordination.
3. Surgical Interventions:
- Severe true LLD or cases causing significant functional limitations may require surgical interventions.
- Procedures include epiphysiodesis (growth plate arrest), limb lengthening surgery, or corrective osteotomies.
4. Monitoring and Follow-Up:
- Regular monitoring of the condition’s progress is essential to ensure that interventions are effective and to adjust the treatment plan as needed.
Apparent Leg Length Discrepancy (LLD):
Definition:
Apparent leg length discrepancy refers to the perceived difference in leg length due to changes in pelvic and spinal alignment, postural factors, or other non-structural causes. Unlike true LLD, apparent LLD is not primarily related to differences in bone length. Instead, it results from variations in how the legs are positioned relative to the pelvis and spine.
Apparent LLD can be influenced by factors such as pelvic tilt, spinal curvature (e.g., scoliosis), and postural adaptations. It is measured by comparing the distance from landmarks on each leg (such as the anterior superior iliac spine or medial malleolus) to the floor, considering postural changes that affect leg positioning. Apparent LLD can impact gait mechanics, muscle imbalances, and overall body alignment.
Causes of Apparent Leg Length Discrepancy (LLD):
- Pelvic Tilt: Changes in pelvic alignment, such as pelvic tilt (anterior or posterior rotation), can create the illusion of leg length discrepancy. A tilted pelvis affects how the legs appear relative to the rest of the body.
- Spinal Curvature (Scoliosis): Scoliosis, a lateral curvature of the spine, can alter the position of the pelvis and affect leg alignment, leading to apparent LLD.
- Muscle Imbalances: Muscle imbalances around the hips and pelvis can cause one hip to be positioned higher than the other, resulting in apparent LLD.
- Postural Adaptations: Poor posture and habits can cause the body to adapt in ways that create an apparent leg length difference.
- Joint Conditions: Conditions affecting the hip joints or sacroiliac joints can influence pelvic alignment and contribute to apparent LLD.
- Soft Tissue Tightness: Tightness in muscles, ligaments, or connective tissues around the hips and pelvis can affect pelvic alignment and leg positioning.
- Functional Leg Length: Functional leg length discrepancy can occur due to factors like hip joint laxity, muscle spasms, or structural imbalances that alter the position of the pelvis and create a perceived leg length difference.
Symptoms of Apparent Leg Length Discrepancy (LLD):
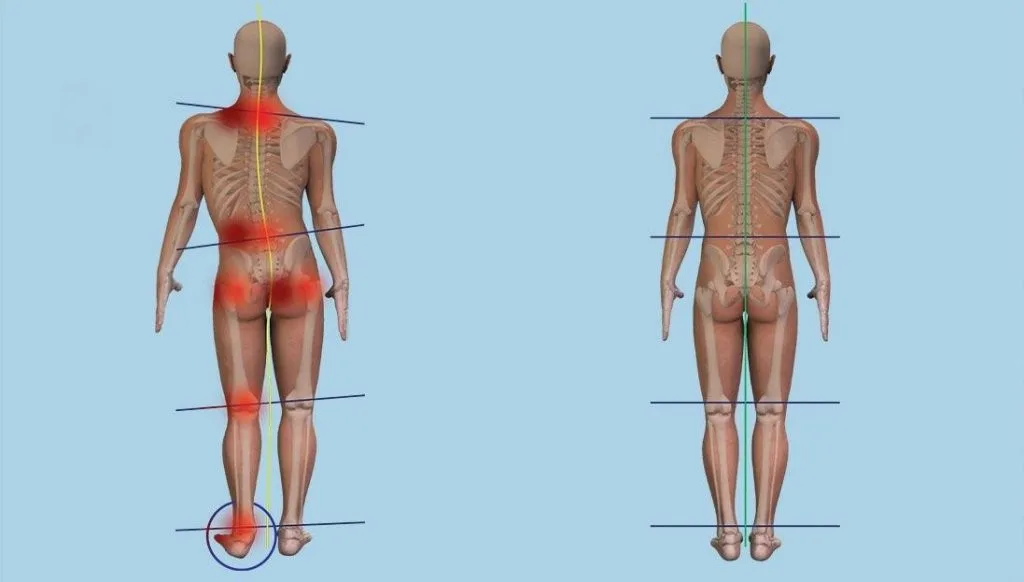
- Postural Changes: Individuals with apparent LLD may exhibit changes in overall posture, such as tilting of the pelvis, uneven shoulders, or a head tilt. This is often due to compensatory adaptations to maintain balance.
- Pelvic Tilt: A common symptom of apparent LLD is pelvic tilt, where one side of the pelvis appears higher or lower than the other. This can lead to muscle imbalances and discomfort.
- Gait Abnormalities: Apparent LLD can cause changes in walking patterns, leading to altered gait mechanics, uneven steps, or a limp as the body adjusts to maintain balance.
- Muscle Imbalances: Muscle imbalances may develop around the hips, pelvis, and lower back due to compensatory movements. This can result in tightness, weakness, and discomfort.
- Low Back Pain: The altered alignment caused by apparent LLD can contribute to low back pain, especially if the pelvis is tilted or the spine is curved.
- Hip Discomfort: Uneven alignment can lead to hip discomfort or pain on one side due to increased stress on the hip joint and surrounding muscles.
- Knee Strain: Altered biomechanics from apparent LLD may place uneven stress on the knee joints, potentially leading to strain, discomfort, or issues like patellofemoral pain.
- Ankle and Foot Issues: Apparent LLD can affect ankle and foot alignment, leading to problems such as overpronation, plantar fasciitis, and Achilles tendon discomfort.
- Fatigue: Muscle imbalances and altered biomechanics can cause certain muscles to work harder, leading to fatigue, especially during prolonged periods of standing or walking.
- Functional Limitations: Depending on the severity of the apparent LLD, individuals may experience limitations in daily activities, sports, or exercise due to altered posture and biomechanics.
- Asymmetrical Clothing Fit: People with apparent LLD might notice that their clothing fits differently on one side of their body due to postural changes.
- Uneven Shoe Wear: Compensatory movements and altered alignment can lead to uneven wear on shoes, with one side of the sole wearing down more quickly.
Measurement of Apparent Leg Length Discrepancy (Apparent LLD):
Apparent leg length refers to the perceived difference in leg length due to factors such as pelvic tilt, spinal curvature, or other postural abnormalities. Unlike true leg length, which measures the actual anatomical bone length. Apparent leg length takes into account changes in pelvic and spinal alignment that can affect the relative positioning of the legs. Here’s a detailed explanation of apparent leg length and the measurement procedure:
Measurement Procedure:
- Patient Positioning:
- The patient should lie down on an examination table in a supine (lying on the back) position.
- The legs should be extended fully and parallel to each other.

2. Locating Bony Landmarks:
- Identify the following landmarks on both sides of the body:
- Anterior Superior Iliac Spine (ASIS): These are the bony projections on the front and upper portion of the pelvis.
- Medial Malleolus: These are the bony prominences on the inner side of the ankles.
3. Measuring Landmarks:
- Using a measuring tape or caliper, measure the distance from each ASIS to the floor (or the examination table surface) on both sides.
- Similarly, measure the distance from each medial malleolus to the floor (or table surface) on both sides.
4. Calculating Differences:
- Compare the measurements of ASIS to floor and medial malleolus to floor for each leg.
- The difference between the ASIS-to-floor measurements and the medial malleolus-to-floor measurements on each side represents the apparent leg length discrepancy.
5. Interpreting the Measurements:
- A positive difference indicates that one leg appears longer than the other due to factors such as pelvic tilt or lumbar curvature.
- A negative difference indicates that one leg appears shorter.
Clinical Considerations:
- Apparent leg length discrepancies can be influenced by postural changes, such as pelvic rotation, lumbar lordosis (swayback), or scoliosis.
- Apparent leg length is influenced by changes in pelvic and spinal alignment, making it a functional measurement rather than an assessment of bone length.
- Doctors use apparent leg length measurements to understand how postural changes affect the perception of leg length. Also use to differentiate between true skeletal discrepancies and functional adaptations.
Accuracy of Measuring Apparent Leg Length Discrepancy (Apparent LLD):
- Moderate Accuracy: Apparent leg length discrepancy measurements are generally accurate in assessing perceived differences due to postural factors.
- Influenced by Postural Changes: Apparent LLD measurements take into account the effects of pelvic tilt, spinal curvature, and other postural adaptations. While they provide insight into perceived differences, they are not direct measurements of bone length.
- Dependent on Patient Positioning: Patient positioning and the examiner’s skill in identifying anatomical landmarks accurately play a role in the accuracy of apparent LLD measurements.
Factors Affecting Accuracy for Both Types:
- Examiner Skill: The accuracy of both types of measurements is influenced by the examiner’s experience and skill in identifying landmarks and using appropriate measurement tools.
- Patient Positioning: Accurate patient positioning is crucial for obtaining reliable measurements in both true and apparent LLD assessments.
- Patient Variability: Anatomical variations among individuals can impact accuracy. For example, variations in the prominence of bony landmarks can affect measurement accuracy.
Clinical Considerations:
- To ensure the highest accuracy, measurements should be taken by qualified healthcare professionals using standardized protocols and appropriate tools.
- For true LLD, accuracy is generally higher due to the direct measurement of bone lengths.
- For apparent LLD, accuracy is influenced by the examiner’s ability to account for postural changes and identify landmarks consistently.
Assessment of Apparent Leg Length Discrepancy (Apparent LLD):
- History and Examination:
- Gather information about the patient’s postural habits, history of spinal conditions (e.g., scoliosis), and any other factors that could influence body alignment.
2. Measurement:
- Measure the apparent leg length by comparing the distance from the ASIS and medial malleolus to the floor (or examination table surface) on each leg.
- Calculate the difference between the measurements to determine the apparent LLD.
3. Postural Assessment:
- Evaluate the patient’s pelvic alignment, spinal curvature, and overall posture to identify any contributing factors to the apparent LLD.
4. Functional Analysis:
- Assess how the apparent LLD affects the patient’s gait, movement patterns, and muscle imbalances.
5. Clinical Considerations:
- Determine whether the apparent LLD is associated with discomfort, altered biomechanics, or compensatory movements.
6. Treatment Planning:
- Develop a treatment plan that addresses the underlying postural issues contributing to the apparent LLD. This may involve physical therapy, exercises, postural correction, and ergonomic modifications.
Management of Apparent Leg Length Discrepancy (Apparent LLD):
- Postural Correction:
- Correcting postural imbalances through physical therapy, exercises, and ergonomic adjustments can help alleviate apparent LLD.
2. Spinal Care:
- If spinal curvature (scoliosis) contributes to the apparent LLD, managing and treating the scoliosis can help improve overall alignment.
3. Muscle Imbalance Correction:
- Targeted exercises to address muscle imbalances around the hips, pelvis, and lower back can help reduce the perceived leg length difference.
4. Posture Awareness:
- Educating the patient about proper posture and providing strategies to maintain good alignment in daily activities is important.
5. Ergonomic Modifications:
- Modifying workspaces, furniture, and footwear to support better posture and alignment can contribute to managing apparent LLD.
6. Physical Therapy and Stretching:
- Stretching exercises can help release tight muscles that contribute to postural imbalances, promoting better alignment.
7. Gait Analysis and Training:
- Gait analysis can identify compensatory movements and abnormal walking patterns, which can be addressed through gait training.
8. Regular Follow-Up:
- Patients with apparent LLD may benefit from regular follow-up appointments to monitor progress and make adjustments to the treatment plan as needed.
Importance of True and Apparent Leg Length Measurement:
The measurement of both true and apparent leg length is of significant importance in the fields of orthopedics, rehabilitation, and musculoskeletal health. These measurements provide valuable information about a person’s anatomy, alignment, and potential underlying conditions. Here’s why true and apparent leg length measurements are important:
1. Accurate Diagnosis:
- True leg length measurements help diagnose structural leg length discrepancies, where one leg is actually shorter than the other due to differences in bone growth or developmental factors.
- Apparent leg length measurements allow clinicians to identify functional leg length discrepancies caused by postural issues, such as pelvic tilt or spinal curvature. Accurate diagnosis is crucial for determining appropriate treatment approaches.
2. Assessment of Leg Length Discrepancy:
- True Leg Length: Accurate measurement of true leg length helps diagnose and quantify leg length discrepancies caused by structural factors, such as bone growth abnormalities. This information guides treatment decisions, such as whether interventions like orthotics or surgical procedures are necessary to address the actual bone length difference.
- Apparent Leg Length: Recognizing apparent leg length discrepancies due to postural factors, such as pelvic tilt or spinal curvature, allows your doctors to differentiate between structural and functional issues. Apparent leg length assessments can help identify whether the discrepancy is related to biomechanical adaptations rather than true bone length differences.
3. Orthopedic Evaluation:
- In orthopedic evaluations, both true and apparent leg lengths are considered when assessing conditions like scoliosis, where spinal curvature can impact pelvic alignment and leg length perception. Understanding these measurements aids in devising appropriate treatment plans, such as bracing or surgical interventions.
4. Differentiation of Causes:
- Understanding the difference between true and apparent leg length helps differentiate between true skeletal differences and postural adaptations. This differentiation guides clinicians in addressing the root causes of leg length issues.
5. Treatment Planning:
- True leg length measurements guide treatment decisions for individuals with genuine bone length differences. Orthotics, lifts, or surgical interventions may be recommended based on the magnitude of the discrepancy.
- Apparent leg length measurements guide treatment for individuals with postural abnormalities. Physical therapy, exercises, and posture correction techniques can be employed to address functional discrepancies.
6. Gait and Biomechanical Analysis:
- Leg length discrepancies can affect gait and biomechanics. Accurate measurements inform healthcare professionals about potential alterations in walking patterns and joint mechanics, helping them design appropriate interventions.
- Both true and apparent leg lengths play a role in gait analysis. Leg length discrepancies can affect walking patterns and lead to compensatory movements. Gait analysis can provide insights into the impact of leg length differences on a person’s overall biomechanics.
7. Customized Care:
- Whether it’s orthotics, prosthetics, braces, or rehabilitation programs, understanding leg length measurements allows for tailored and personalized care that addresses each patient’s specific needs.
- For individuals with leg length discrepancies, orthotists and prosthetists use leg length measurements to create custom devices that restore balance and proper alignment. To ensure optimal fit and functionality, accurate measurements are essential.
8. Prevention of Complications:
- Unaddressed leg length discrepancies can lead to musculoskeletal imbalances, joint strain, and even chronic pain. Proper measurement and subsequent management can help prevent these complications.
9. Surgical Interventions:
- Surgeons use true leg length measurements to plan procedures such as limb lengthening or correction of bone deformities. Accurate measurements are essential for achieving the desired surgical outcomes.
10. Monitoring Progress:
- Serial measurements of leg length are important for tracking progress in patients undergoing interventions. Monitoring helps ensure that the chosen treatment approach is effectively addressing the leg length issue.
11. Rehabilitation Optimization:
- Physical therapists and rehabilitation specialists use leg length measurements to design targeted exercises that restore muscle balance and functional alignment.
- When designing rehabilitation programs, physical therapists consider leg length measurements to tailor exercises that address muscle imbalances and gait abnormalities. Accurate assessment of leg length helps optimize the effectiveness of therapeutic interventions.
In essence, both true and apparent leg length measurements are critical tools that guide medical professionals in diagnosing, treating, and managing a range of conditions affecting the lower limbs. These measurements enable individualized care plans that address each patient’s unique needs and promote optimal musculoskeletal health and function.
Clinical Significance:
- Both true and apparent leg lengths are important in assessing and diagnosing musculoskeletal issues.
- An apparent leg length discrepancy doesn’t necessarily indicate a true bone length difference; it might be due to postural changes. Therefore, healthcare professionals need to differentiate between true and apparent leg length when evaluating patients.
- Leg length discrepancies, whether actual or apparent, can lead to gait abnormalities, altered biomechanics, and potential strain on the musculoskeletal system.
- Accurate measurements of both true and apparent leg lengths, along with a thorough physical examination and possibly imaging studies, help clinicians determine the underlying causes of leg length discrepancies and related issues.
Difference between true and apparent Leg Length Discrepancy(LLD)
True LLD involves actual differences in bone lengths between the legs, while apparent LLD is caused by non-structural factors affecting alignment and posture.
The primary distinction lies in the nature of the cause. True LLD originates from structural bone length differences, while apparent LLD arises from non-structural factors that alter body alignment.
True LLD is accurately measured by directly assessing bone lengths. Apparent LLD is measured by evaluating the perceived positioning of anatomical landmarks.
True LLD’s impact is related to biomechanics and bone health, whereas apparent LLD’s impact is related to functional adaptations and postural imbalances.
When there is a true leg length discrepancy, the patient’s two lower extremities actually differ in length from the FEMORAL head to the plantar surfaces of the feet. A functional leg length discrepancy, also known as an apparent leg length discrepancy, occurs when a patient has two lower limbs that are the same length from the femoral heads to the plantar surfaces of the feet, but one lower limb appears differently than the other due to other conditions like joint or muscle contractures.
True leg length discrepancy refers to the actual difference in anatomical bone length between the two legs and Apparent leg length discrepancy refers to the perceived difference in leg length due to postural factors, pelvic tilt, or spinal curvature.
Difference in etiology: True leg length discrepancies are primarily due to variations in bone growth, congenital conditions, fractures, or surgical procedures that affect bone length and Apparent leg length discrepancies are caused by changes in pelvic and spinal alignment, leading to variations in how the legs are positioned relative to the pelvis and spine.
- True LLD is a direct reflection of differences in actual bone lengths and can lead to biomechanical issues and gait abnormalities.
- Apparent LLD is related to postural imbalances and functional adaptations, leading to changes in leg alignment without necessarily altering bone lengths.
Key Differentiation in symptoms:
- True LLD: Symptoms are influenced by actual differences in bone lengths, leading to biomechanical and joint issues.
- Apparent LLD: Symptoms are primarily related to postural changes, muscle imbalances, and altered biomechanics due to functional adaptations.
Different Measurement: True leg length is measured from a fixed point on the pelvis (ASIS) to a specific landmark on the ankle (medial malleolus) on each leg and Apparent leg length is measured by comparing the distance from landmarks on each leg (ASIS or medial malleolus) to the floor, which takes into account postural changes.
- In true LLD measurement, the distance between the ASIS and medial malleolus is measured directly, providing a quantifiable difference in bone length.
- In apparent LLD measurement, the focus is on the relative positioning of anatomical landmarks (ASIS and medial malleolus) to the floor, considering pelvic tilt, spinal curvature, and postural factors.
Accuracy comparison: True leg length is a more accurate representation of leg length because it directly measures the bone lengths. Apparent leg length can be influenced by postural factors and is a functional measurement that reflects perceived differences rather than true bone length.
- For true LLD, accuracy is generally higher due to the direct measurement of bone lengths.
- For apparent LLD, accuracy is influenced by the examiner’s ability to account for postural changes and identify landmarks consistently.
True leg length discrepancies can lead to biomechanical issues, altered gait patterns, and potential joint problems. They are often assessed using imaging (X-rays) and are addressed with interventions like lifts, orthotics, or surgical procedures and Apparent leg length discrepancies may lead to compensatory movements, altered gait mechanics, and muscle imbalances. They are often addressed through physical therapy, postural correction, and exercises aimed at improving alignment.
- The assessment of true LLD involves measuring bone lengths, evaluating skeletal growth, and considering factors such as fractures or surgeries.
- The assessment of apparent LLD involves considering postural changes, spinal alignment, muscle imbalances, and other factors influencing leg positioning.
Key Differences:
- True leg length discrepancy is a result of actual bone length differences, whereas apparent leg length discrepancy is influenced by postural changes and alignment.
- True leg length is measured from a fixed point to the ankle, while apparent leg length considers the effects of pelvic and spinal alignment on perceived leg length.
- True leg length discrepancies often require interventions to address biomechanical issues, while apparent leg length discrepancies are typically managed through postural correction and exercises.
In summary, true leg length discrepancy relates to actual bone length differences, while apparent leg length discrepancy relates to the perceived difference caused by postural changes. Both discrepancies can impact musculoskeletal health and require appropriate assessment and management strategies.
True leg length discrepancy pertains to actual differences in bone length. Apparent LLD relates to perceived differences due to postural and alignment factors. Both types of discrepancies can have implications for musculoskeletal function. may require appropriate assessment and management strategies based on their underlying causes.
FAQs:
True LLD involves actual differences in bone lengths between the legs. Apparent LLD is caused by non-structural factors affecting alignment and posture.
It is measured from a fixed point to the ankle. Apparent leg length considers the effects of pelvic and spinal alignment on perceived leg length.
True leg length discrepancies often require interventions to address biomechanical issues. Apparent leg length discrepancies are typically managed through postural correction and exercises.
True LLD is measured by directly assessing bone lengths using fixed anatomical landmarks. Apparent LLD is measured by evaluating the relative positioning of landmarks to the floor, considering postural changes.
True LLD can result from unequal bone growth, congenital conditions, fractures, surgical interventions, or bone disorders bone disorders, like osteomyelitis (bone infection) or osteochondroma (benign bone tumor) affecting bone length. Variations in the rate of bone growth during childhood and adolescence.
Apparent LLD is primarily caused by factors such as pelvic tilt, spinal curvature (scoliosis), muscle imbalances, and postural adaptations.
True LLD can lead to altered gait patterns, joint stress, and musculoskeletal issues due to structural differences. Apparent LLD primarily impacts posture, muscle balance, and gait mechanics due to functional changes.
Yes, true LLD can often be managed with custom-made orthotics or shoe lifts to equalize leg lengths and improve alignment.
Surgery is generally not needed for apparent LLD since it is related to postural and functional factors. Treatment involves addressing the underlying causes through physical therapy, exercises, and postural corrections.
While it’s challenging to diagnose accurately at home. True LLD might show differences in leg length when lying down. Apparent LLD might be influenced by postural changes when standing.
Both types of discrepancies can contribute to discomfort or pain, especially if left untreated. Effective treatment can reduce these symptoms.
Yes, non-surgical interventions like physical therapy, exercises, orthotics, and postural correction can often effectively manage both true and apparent LLD.
Leg length discrepancies are relatively common and can vary in severity. Minor discrepancies might not cause noticeable issues, while larger discrepancies might impact daily activities and biomechanics.
Diagnosis involves a thorough medical history, physical examination, measurements, imaging (such as X-rays), and assessment of gait and posture.
Yes, both true and apparent LLD can affect biomechanics and potentially impact sports performance. This leading to imbalances, altered mechanics, and increased risk of injuries.
Yes, apparent LLD can lead to gait problems. Like compensatory movements, altered gait mechanics, and muscle imbalances due to changes in posture and alignment.
True LLD Symptoms are influenced by actual differences in bone lengths, leading to biomechanical and joint issues. Apparent LLD are primarily related to postural changes, muscle imbalances, and altered biomechanics due to functional adaptations.





