
Rotator cuff injury Test
Rotator cuff injury test helps to diagnose and to differentiate from other similar shoulder pain-related conditions. It is also used to examine for full-thickness rotator cuff tears, mainly the supraspinatus.
Table of Contents
Definition
- A significant tear in the rotator cuff is hard to define precisely. The number of torn tendons and sometimes the size of the tear can both indicate the severity.
- Lädermann and co suggested that When at least two tendons are completely torn, it is considered a complete rupture of a rotator cuff tear.
At least one of the two tendons must retract beyond the humeral head, regardless of the number of torn tendons.
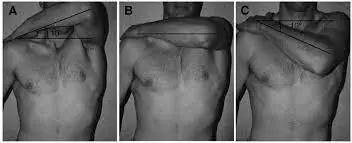
According to Collin et al., there are five additional types of rotator cuff tears: - Type A: tears of the supraspinatus and superior subscapularis
- Type B: tears of the entire subscapularis and supraspinatus
- Type C: tears of the supraspinatus, superior subscapularis, and infraspinatus supraspinatus and infraspinatus tears
- Type D: tears of the supraspinatus and infraspinatus
- Type E: Other authors refer to supraspinatus, infraspinatus, and teres minor tears as rotator cuff tears that involve one or more of the four tendons that make up the rotator cuff. The M. supraspinatus tendon is the most frequently affected. The size, location, and form of rotator cuff tears can be described using a variety of classification systems. Typically, tears are described as either partially or completely thick. The system of classification is:
- A tiny tear: less than one cm
- Moderate tear: 1–3 cm
- Big tear: 3–5 cm
- Large tear: exceeding 5 cm.
Tests for the Subscapularis
Internal Rotation Lag Sign
- The goal of these tests is to look for tears in the Subscapularis tendon in the rotator cuff.
- Method of performing this test
The patient is seated, and the examiner is behind them. Behind the back, the affected arm is brought into maximum internal rotation (the hand of a patient against the lumbar region). - The patient’s forearm and hand are moved away from the back while the examiner controls the patient’s arm at the elbow and wrist/hand, which are passively brought into 20 degrees of extension. While the examiner maintains support at the elbow, instruct the patient to actively maintain this position.
- A tear in the subscapularis tendon is indicated by a lag. Using 5-degree intervals, describe the magnitude of the lag, with a noticeable drop indicating a large or massive tear and a smaller lag indicating a partial tear.

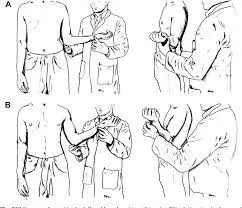
Belly Press Test
- The purpose of the belly press test is to isolate the subscapularis muscle and check for tears or dysfunction in the subscapularis muscle. When the lift-off test isn’t possible due to pain or a limited range of motion in the shoulder’s internal rotation, it is frequently used in its place.
- How to perform this test
- The patient sits or stands with their elbow bent 90 degrees and their palm on their upper abdomen, just below the xiphoid process.
- Through internal rotation of the shoulder, the patient is instructed to press the palm of their hand against their abdomen.
- If the patient compensates for the movement through initiated wrist flexion, shoulder adduction, and shoulder extension, the test indicates that the subscapularis muscle is dysfunctional.
- The elbow would drop behind the trunk as a result of this unconscious compensatory movement.

Belly-Off Sign
- The belly press test can be used to evaluate the subscapularis muscle when the Internal Rotation Lag Sign (IRLS) or lift-off test cannot be performed due to a lack of range of motion or pain.
- Test to remove: With the hand on the lumbar region, the arm is extended with an internal rotation. The patient is instructed to lift the arm posteriorly from this position.
- Sign of internal rotation lag: The arm is rotated almost completely internally with the same starting position as above. After that, the hand’s dorsum is lifted completely away from the body until the internal rotation is complete. After that, the patient is asked to actively hold this position. A shortage between the effectively kept up with range and the latently put range demonstrates the test is positive.
- How to perform this test
The subject is instructed to press the abdomen with a flat hand while maintaining maximum internal rotation of the arm.
If only shoulder extension and wrist flexion exert pressure, the Inference Test is positive if the elbow drops posteriorly, indicating a loss of internal rotation. The Napolean sign refers to this position. - Properties The belly-off sign is a promising new clinical tool for patients with intact external rotators, subtle subscapularis tendon lesions, and postoperative subscapularis weakness.
The belly-off sign loses its diagnostic value when there are no external rotators because it becomes negative.
Bear Hug Test
- Objective
- The subscapularis muscle is a major component of the rotator cuff. It also forms the anterior part of the force couples of the glenohumeral joint and provides 50% of the rotator cuff’s strength.
- The subscapularis muscle tear or dysfunction can be checked for with the bear hug test.
- Technique
- The patient performs the technique by placing the affected side’s palm on the opposite shoulder, with the fingers extended and the elbow facing the body.
- The patient is instructed to keep their arm in that position. The patient resists the therapist by performing internal rotation after the therapist applies an external rotation resisting force perpendicular to the forearm.
- If the patient showed weakness in resisted internal rotation of more than 20% to the opposite side, or if they were unable to maintain the hand against the shoulder, the test is positive.
Tests for the supraspinatus and infraspinatus
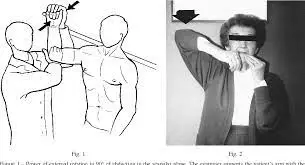
External rotation lag sign
- Purpose
Hertel et al. first described the external rotation lag sign (ERLS) in 1996. The diagnosis of a full-thickness rotator cuff tear is the focus of this clinical diagnostic test. The supraspinatus and infraspinatus tendons’ integrity will primarily be evaluated using the ERLS. - Methodology
- The ERLS is carried out while the patient is seated. To prevent elastic recoil of the joint capsule and the scapulothoracic joint, the elbow is passively flexed to 90 degrees, and the shoulder is abducted to 90 degrees and held 5 degrees off maximal external rotation.
- The examiner then asks the patient to actively maintain the position while maintaining support through the elbow and releasing the wrist. A full-thickness tear of the rotator cuff would be indicated by the inability to maintain the position (lag).
- The degree of the lag is measured to the nearest 5 degrees. The contralateral side serves as a control, particularly for evaluating minute lags that could be caused by excessive external rotation or hyperlaxity by the examiner.
- Pathologic changes in the glenohumeral joint’s passive range of motion (PROM) can make testing and interpreting difficult. For instance, false-negative and false-positive outcomes can be anticipated when PROM is decreased by capsular contracture or increased by subscapularis rupture.
Jobes Relocation Test
- Purpose
The purpose of the Jobe Relocation Test, which is also known as the Fowler Sign, is to check for glenohumeral joint anterior instability. - Technique
This test is very similar to the Apprehension Test and is often given after the Apprehension Test to find out what happened if a positive result came back. The patient is lying in a supine position, with their elbows flexed to 90 degrees and their head lowered to 90 degrees. - After that, the therapist applies an external rotation force to the shoulder; the Apprehension Test is deemed positive if the patient expresses apprehension in any way. If the patient’s anxiety or pain decreases in this position, the Jobe Relocation Test is considered to be positive.
- At this point, the therapist may apply a force to the shoulder that is directed posteriorly. In order to reduce the risk of shoulder dislocation, the therapist should always bring the arm back into a neutral position before releasing the relocation force (the posterior glide of the head of the humerus).
- In the event that the patient’s side effects decline or are dispensed with while playing out the Jobe Movement
- Test, the potential judgments include: subluxation, dislocation, or impingement of the glenohumeral
- The diagnosis may include pseudo laxity or anterior instability of the GH joint, or possibly the scapulothoracic joint if the apprehension predominates during the Crank Test and goes away during the Jobe Relocation Test.
- A secondary impingement or a posterior SLAP labral legion should also be taken into consideration.

Drop Arm Test
- Purpose
The purpose of the drop arm test is to check for full-thickness rotator cuff tears, especially those of the supraspinatus. This can help distinguish between rotator cuff pathologies and shoulder pain syndrome, also known as shoulder impingement. - Utilizing the drop arm test as part of a series of tests, such as:
- A series of tests will help distinguish between rotator cuff muscles and provide a more precise diagnosis. These tests include the empty/full can test, the external rotation lag sign, the internal rotation lag sign, and the Hornblower’s sign.
- Technique
- From behind the patient who is seated, passively abduct the patient’s arm to 90 degrees and full external rotation while supporting the arm at the elbow. Then, ask the patient to slowly lower the arm back to neutral.
- Interpretation
- If the patient is able to control slowly lowering the arm without experiencing symptoms, the test is negative.
- It is a positive test if the arm drops suddenly or if there is weakness in keeping the arm in the right position during the eccentric part of abduction. There may also be pain while the arm falls, which could mean that the supraspinatus has been torn all the way through.

Test for a Teres minor tear
Hornblower’s Signage
- Objective: To check for a Teres minor tear.
- How to perform this test
The patient is either seated or standing. The examiner flexes the patient’s elbow 90 degrees while putting the patient’s arm in a 90-degree scapular plane. - The next step is to force the patient to externally rotate. If the patient is unable to rotate their body externally, the test is positive.
Full-Thickness Rotator Cuff Tear
Painful Arc
- Painful Arc is to identify potential subacromial impingement syndrome. A positive result on the painful arc, like the majority of special tests, is not necessarily indicative of subacromial impingement.
- How to perform this test
A patient may be instructed to abduct an arm in a scapular plane during sitting or standing. A patient must inform the physiotherapist of any pain they are experiencing in or around the glenohumeral joint while abducting the arm. - A physical therapist may instruct a patient to continue abducting an arm as high as possible once the pain starts. The amount of pain that the patient is feeling should go down once they reach about 120 degrees of abduction.
- The patient should slowly reverse the motion after completing the abduction and use the adduction movement to return the arm to its neutral position. If the patient experiences pain between 60 and 120 degrees of abduction, which diminishes after 120 degrees of abduction, this test is deemed positive.
Infraspinatus Test
- Purpose
Purpose of the Infraspinatus Test One of the rotator cuff muscles is the infraspinatus muscle. Shoulder impingement is caused by dysfunction in the rotator cuff muscles because the head of the humorous superiorly moves when the arm is raised. - The infraspinatus muscle is frequently involved in shoulder conditions like rotator cuff tears and impingement.
- The Infraspinatus test is used to look for the involvement of the infraspinatus muscle in rotator cuff disorders like subacromial impingement or rotator cuff tears.
- How to perform this test
The patient should have his elbows flexed to 90 degrees and his arms at his side, not quite touching his trunk. The examiner touches the patient’s hands’ dorsum with one hand. The examiner resists the patient’s request to externally rotate both forearms. The patient can do this. - When there is pain or weakness in external rotation, the test is positive. Infraspinatus tears are normally easy so outside pivot shortcoming emphatically recommends infraspinatus tears.
FAQs
The following are the most typical signs of a rotator cuff tear: Pain at rest and at night, especially when lying on the shoulder that is hurt. Pain when you lift and lower your arm or perform particular movements. Inability to lift or rotate your arm.
The first step in this test is to place the injured arm behind your back while resting your hand on your lower back.
Now, try to lift your arm off your back. If you feel pain or weakness when you try to lift your hand off your back, it could be a rotator cuff injury.
The muscle usually separates from the bone, either partially or completely, in most rotator cuff tears. Tears in the rotator cuff cannot heal on their own. Your shoulder joint can be restored with rotator cuff surgery. For rotator cuff injuries, the best doctor to see is a shoulder surgeon.
MRI: Medical professionals are able to get a better look at soft tissue injuries thanks to the images that are produced by a magnetic resonance imaging test. These are helpful for determining whether the shoulder’s ligaments and tendons have been damaged. CT check: Using specialized X-ray equipment.
In most cases, the pain will radiate down the side of your arm from the front of your shoulder. It might be present when doing overhead tasks like lifting or reaching (like serving in tennis or painting the ceiling, for example). When you try to sleep on the affected side, you might feel pain.




