Rehabilitation for Biceps Tendonitis
Rehabilitation plays a crucial role in the management of biceps tendonitis, aiming to reduce pain, promote healing, restore strength and flexibility, and prevent future injury.
Table of Contents
What is Biceps Tendonitis?
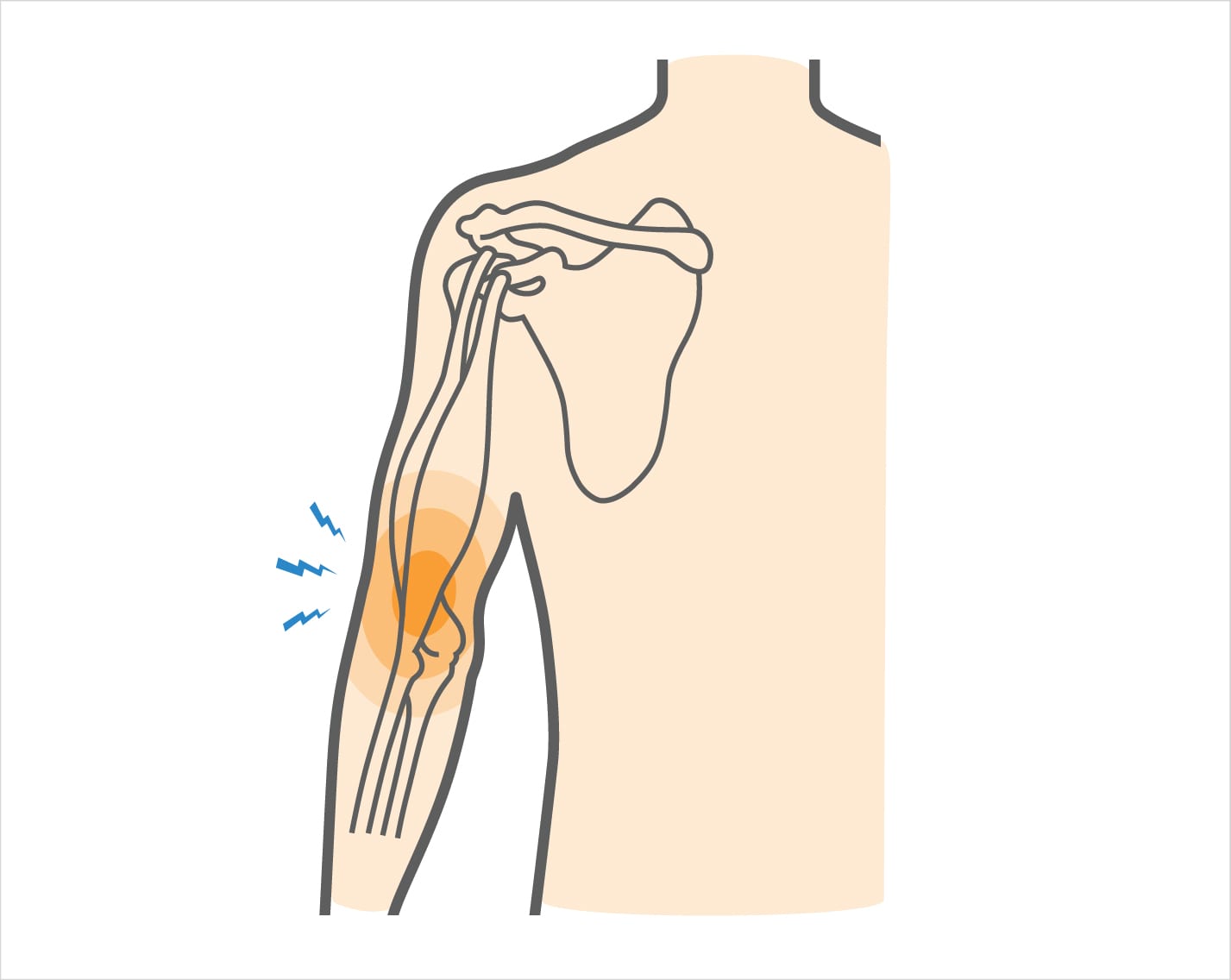
Inflammation of the biceps tendon sheath (lining) or strain on the upper biceps tendon is the two main causes of proximal biceps tendonitis and tenosynovitis, which causes pain in the front of the shoulder and upper arm. A substance that lubricates the tendon is secreted by the lining. The tendon cannot move freely within its sheath when the lining is irritated. The biceps tendon is one of the anchor points for the biceps muscle, which is necessary for bending the elbow and twisting the wrist. Additionally, it affects how the shoulders work.
- A grade 1 or 2 tendon strain could be present in proximal biceps tendinitis.
- Grade 1: Mild strains are classified as grade 1. Although there is tiny tendon tearing, there is only a small pull of the tendon. The tendon is the right length, and there is no loss of strength.
- Grade 2: An average strain is a grade 2 strain. At the bone-tendon or muscle-tendon junction, tendon fibres within the tendon’s material are torn. Strength typically decreases when the tendon’s length or the entire muscle-tendon-bone unit lengthens.
- Grade 3: A tendon that has completely ruptured has a grade 3 strain.
Anatomy of the Biceps:
The upper arms’ front surfaces contain the biceps muscles. Near the shoulder joint, they originate from two heads (thus the term “biceps”). The shoulder blade’s coracoid process is where the short head of your biceps originates. A synovial sheath surrounds the long head of the biceps, which starts from the supraglenoid tubercle of your shoulder joint. This tendon sheath gives it lubrication so that it can move freely at the front of your upper arm. The radial tuberosity of your forearm is where the biceps muscle inserts after traveling down the upper arm.
In addition to helping move your shoulder joint and assisting the rotator cuff muscle group in maintaining the front of your shoulder, your biceps also work to turn your forearm into a palm-up position. Biceps tendonitis can develop as a result of the biceps tendon being overloaded at the elbow or shoulder.
Causes:
- The strain brought on by a rapid increase in activity level or intensity
- A direct hit or shoulder injury
- Recurrent damage to the biceps muscle-tendon unit makes it more likely
- Combined with rotator cuff inflammation or injury, as well as other shoulder issues Sports that entail contact, throwing, gymnastics, weightlifting, and bodybuilding have an increased risk.
- Heavy labour
- Poor physical condition (strength and flexibility)
- Inadequate warm-up prior to game or practice
Symptoms of Biceps Tendonitis:
There are many symptoms of possible biceps tendonitis. These may include:
- Pain in your upper arm and shoulder
- The upper part of the arm and shoulder in the front are tender to the touch.
- Swelling
- Warmth
- Redness over the front of the shoulder
- Difficulty lifting your arm up
- Feelings of weakness in the arm
- Shoulder and elbow mobility and function against resistance exacerbate the pain
- Limited motion of the shoulder or elbow
- A crackling sound is generated when moving or touching the tendon or shoulder
Visit your doctor as soon as possible to get a diagnosis if you think you may have biceps tendonitis. You can then be certain to begin receiving the appropriate care for your condition.
Diagnosis:
Performing a clinical examination of your shoulder, elbow, and upper arm is necessary to make the diagnosis of biceps tendonitis. To see the soft tissue structures surrounding your shoulder, your doctor may arrange diagnostic procedures like magnetic resonance imaging (MRI). Biceps tendonitis may be confirmed (or ruled out) by this.
Since various disorders can cause anterior shoulder pain, biceps tendonitis may be challenging to diagnose. These can include a torn rotator cuff, arthritis in the AC joint, a torn labrum in the shoulder, or cervical (neck) radiculopathy.
Diagnosis Criteria
The following requirements must be met in order for biceps tendinopathy to be diagnosed:
- Tendon sheath enlargement (as reported by Schmidt et al., transverse view: 4.6 mm for women, 5.5 mm for men, longitudinal view: 2.5 mm for women, 2.8 mm for males)
- According to Bruyn et al., tendon sheath fluid accumulation is an aberrant buildup of isoechoic or hyperechoic intraarticular material that is less than three millimeters in diameter and is displaceable and compressible. Increased colour flow signals around the enlarged biceps tendon were recognized as important to a biceps tendinopathy diagnosis in addition to the diagnostic criteria.
- These diagnostic standards were agreed upon by all parties engaged in the musculoskeletal US examination in order to prevent operator-dependent misdiagnosis.
Treatment for Biceps Tendonitis
An initial evaluation is the name of your first visit with a physical therapist (PT) for biceps tendonitis. Your PT will ask you questions regarding your injuries during this appointment. They will inquire into the circumstances surrounding your accident, how it is affecting your daily life and leisure time, and whether you have received any medical attention thus far. Your PT will also inquire about your medical background and possibly go over any medications you are currently taking.
Your physical therapist will do a number of tests and measurements during the PT evaluation for biceps tendonitis. These are completed in order to establish your functional baseline and direct shoulder treatment. The following tests are frequently carried out during a biceps tendonitis evaluation:
- Palpation
- Range of motion (ROM)
- Strength
- Special shoulder tests
- Functional mobility
Your PT will go over your treatment plan with you after evaluating your condition and finishing the evaluation. Goals will be established, and your biceps tendonitis therapy can start.
Medication:
Inflammation is reduced with nonsteroidal anti-inflammatory drugs, such as aspirin and ibuprofen (do not take within 7 days following surgery). Take them as your doctor has prescribed. If you have any bleeding, stomach discomfort, or symptoms of an allergic reaction, call your doctor right once. Acetaminophen and other non-prescription painkillers may also be utilized.
Typically, painkillers are not prescribed for this disease. Use the medication only as prescribed and in the quantity that you require.
Injections of cortisone lower inflammation, and anaesthetics block pain signals momentarily. However, these are only used in the most severe situations; cortisone dosages are limited since they might damage muscle and tendon tissue.
Physical Therapy Treatment for Biceps Tendonitis:
Biceps tendonitis can be treated using a wide range of techniques and modalities. These are intended to assist in reducing pain and inflammation, enhancing range of motion and strength, and enhancing arm and shoulder function without discomfort.
Stretching and strengthening exercises are utilized as the first line of treatment, along with medications and cold packs to reduce pain. The activity that first triggered the issue is also changed. All of them can be done at home, though consulting a physical therapist or athletic trainer may be advised. It might be advised to administer a cortisone injection to the area surrounding the tendon (inside the sheath). Surgery is typically not required and is typically only contemplated after at least six months of conservative treatment, either to remove the inflammatory tendon lining or to detach the deteriorated tendon and re-insert it into the arm bone. Before performing surgery for the tendinitis itself, it may be advised to address underlying shoulder issues that may be causing it.
Exercise:
Exercise should be your primary method of biceps tendonitis treatment. Exercise has been demonstrated to assist increase your arm’s and shoulder’s range of motion (ROM), strength, and functional mobility. Additionally, it helps promote healing by enhancing blood flow to the tendon.
Your rehabilitation program for biceps tendonitis may involve a variety of exercises, such as:
Exercises for shoulder range of motion (ROM) can be passive, in which case the physical therapist moves your arm and shoulder, active assistive, in which case you move your shoulder with the aid of an external device, or active. Range of motion:
Exercises that increase range of motion can help with shoulder mobility and function as well as provide your biceps tendon with some much-needed movement.
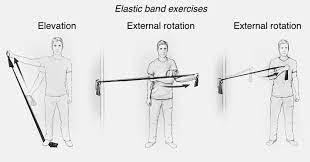
- Strengthening of the rotator cuff:
Your physical therapist might suggest activities to strengthen those muscles if they believe that your biceps tendonitis is being brought on by rotator cuff weakness. Exercises could involve an active range of motion with a free weight, internal and external rotation with a resistance band, or the “empty can” exercise. The ideal workouts for your condition can be demonstrated to you by your PT.
- Stabilized scapula:
Both your long and short biceps tendons attach to your shoulder blade (scapula), and an unnaturally positioned scapula may be to blame for your biceps tendonitis. Your biceps tendinopathy may be treated with exercises aimed at improving your scapula’s neuromuscular control
Scapular stabilizing exercise helps to stabilize the scapula and increases muscle strength.
- Exercise for endurance:
Your therapist might suggest that you work on enhancing upper-extremity endurance while you’re in the PT clinic. This can improve the movement and functionality of your shoulder by increasing blood flow to the biceps tendon and shoulder. An upper body ergometer could be useful, and a rowing machine could help with shoulder endurance.
According to some research, eccentric exercise may be beneficial for tendinopathy and biceps tendon issues. Exercises known as eccentrics involve contracting the biceps muscle and tendon as they extend. According to one theory, this kind of contraction changes the collagen that makes up the tendon, promoting appropriate healing.
You can also be required to follow a self-directed home exercise regimen by your physical therapist. You can keep up the gains you make in the clinic with the help of these workouts.
Exercise for biceps tendonitis needs to be difficult but not uncomfortable. You need to stop exercising and consult your PT if any exercise causes pain to worsen.
Massage:
For your biceps tendonitis, your physical therapist may use a variety of massage treatments. To encourage collagen development around your torn tendon, try a cross-friction massage. This may lessen discomfort and enhance regional blood flow. Your shoulder and arm may be able to move more freely as a result of massage-induced tissue mobility improvement.
Kinesiology tape:
Kinesiology taping, often known as K-tape, is a therapeutic method that certain physical therapists employ. Your upper arm or shoulder will be taped with flexible fabric tape by your physical therapist. The tape is applied to reduce pain and muscle spasms or to promote healthy muscle function.
A word of caution: K-tape is a more recent PT procedure, and it hasn’t been shown to be successful in treating tendon issues. The tape has reportedly helped some people with their symptoms and function, although no rigorous scientific testing has been done on it yet.
Heat:
If you have biceps tendonitis, your physical therapist may use heat on your upper arm and shoulder.
Before engaging in stretching and strengthening exercises recommended by your doctor, physical therapist, or athletic trainer, heat may be applied. Use a heating pad or a warm bath.
The increased blood flow brought in by the heat flushes out any waste products that may have accumulated due to inflammation while also bringing in oxygen and nutrients. Additionally, the use of heat can reduce discomfort and increase tissue mobility. A couple of layers of towelling should be placed between the hot pack and your skin to prevent burns from occurring from the heat. If you become excessively warm during heat treatment, let your PT know.
Ice:
Biceps tendonitis can be treated by applying ice. Cold therapy is used to treat both acute and chronic pain by reducing inflammation. For inflammation and pain, using cold for 10 to 15 minutes every 2 to 3 hours is recommended. You should also apply cold right away after any activity that makes your symptoms worse. Use ice massages or ice packs. Ice can be used to reduce localized pain, oedema, and inflammation because it reduces blood flow. At the conclusion of your therapy session, your PT could apply ice to reduce inflammation. Since putting ice directly on your skin could result in a frost burn, caution should be taken. If you experience any discomfort while using ice at the PT clinic, let your therapist know.
Ultrasound:
Physical therapy clinics have long used ultrasound technology. Your wounded tissue is treated by having an ultrasonic wand with a coupling gel passed over it for five to ten minutes. The wand heats the tissue by delivering ultrasonic waves to your biceps tendon.
You shouldn’t experience anything throughout an ultrasound procedure than a slight heat around the ultrasound head. If ultrasound is not used correctly, one could experience a burning feeling. If you have any pain, let your PT know so that changes can be made.
Despite the fact that ultrasound has been used for a long time in physical therapy, numerous studies have indicated that it is ineffective when compared to alternative treatments, such as strenuous exercise. Due of this lack of advantages, ultrasonography is not commonly used by physical therapists. Even so, some therapists employ it, and you might come across it if you’re getting treatment for biceps tendonitis.
Electrical stimulation
You could utilize electrical stimulation to treat tendinopathy or tendonitis in your biceps. The stimulation, also known as e-stim, can be used to lessen discomfort, enhance muscle performance, or boost circulation. Two to four tiny electrodes will be positioned around your shoulder and upper arm, and electricity will be applied to the electrodes if your physical therapist decides to utilize e-stim to treat your biceps tendonitis. Although it could irritate a little, this electrical impulse shouldn’t hurt. The majority of e-stim procedures, such as neuromuscular electrical stimulation (NMES) and transcutaneous electric neuromuscular stimulation (TENS), last between 10 and 20 minutes.
Dry Needling:
Similar to acupuncture, the physical therapy procedure known as “dry needling” involves putting tiny needles into tendons.1 The needle aids in improving localized blood flow while reducing pain and muscular spasm. There hasn’t been much research on dry needling because it’s a new treatment.
Iontophoresis:
Iontophoresis, which uses electricity to deliver medication via your skin and into your wounded biceps tendon, is a unique type of electrical stimulation. The drug is often a negatively charged anti-inflammatory liquid. The medication is repelled by a direct current that is also negatively charged, which forces the medication into your tendon.
Iontophoresis typically lasts 10 to 20 minutes and shouldn’t hurt. After the iontophoresis is finished, you can experience some tingling underneath the medicated electrode and some skin redness.
Iontophoresis has been demonstrated to be useful in treating tendon issues, although other research does not back up its usage as an anti-inflammatory therapy. Make sure you are aware of what to expect from iontophoresis, and ask your physical therapist any questions you may have.
Range of motion exercise:
These are a few of the first exercises you’ll do as part of your rehabilitation program up until your doctor, physical therapist, or sports trainer certifies that the symptoms have subsided. Please
- Flexible tissue can withstand more pressure when engaged in activities.
- Each stretch needs to be maintained for
- There should be a little stretching sensation
- Flexion:
Method 1: SHOULDER FLEXION

- Lay flat on your back. In your Left hand, firmly grasp the bottom of a stick, an umbrella’s handle, or a golf club’s blade.
- Raise your arm overhead as shown while holding the stick until you feel a light stretch. The thumb should be used as a “thumbs up” sign when leading.
- Exercise two more times each day. every repetition for 30 seconds.
- Lie on the back with your hands shoulder-width apart and a stick in each hand.
- Raise both hands above your head till a light stretch is experienced.
- Perform the exercise twice daily. 30-second holds between each repetition

Method 2: SHOULDER FLEXION
- As you are demonstrating, carefully “walk” your fingers up the wall as you are standing close to it until you feel a slight stretch.
- Perform the workout twice daily. Hold for 30 seconds between each repetition.
Abduction:
Method: SHOULDER ABDUCTION
- As shown, lay on your back while gripping a stick, umbrella handle, or golf club in each hand. A “thumbs up” gesture should be made with the hand.
- Using the stick, gradually move your arm as high aloft and away from your side as you can without experiencing pain. Push until a light stretch appears.
- Perform the exercise twice daily. every repetition for 30 seconds.
Internal Rotation:

Method 1:Shoulder Internal Rotation
- As indicated, place a stick in your back and grasp it with both hands.
- Move the stick up your back until a light stretch is felt.
- Exercise two more times each day. Hold for 30 seconds between each repetition.

Method 2: Internal Rotation Shoulder
- Your hand should be behind your back.
- With the hand behind your back, grab a towel and drape it over the shoulder on the opposite side of you.
- Pull your hand deeper up your back using the cloth until you feel a light stretch.
- Perform the exercise twice daily. Hold for 30 seconds between each repetition.
STRENGTHENING OF SHOULDER FLEXION
Method 1: Flexing the shoulders
- Hold the rubber band/tubing, or stand holding a weight in your hand.
- As far as you can raise your arm upward without experiencing any pain, slowly. Avoid “shrugging up” your shoulder when performing this exercise.
- Maintain the “thumbs-up” gesture with your hand.
- Maintain this posture for 30 seconds, then slowly resume your original position.
- Perform the workout twice daily.
Method 2: Isometric shoulder flexion
- Raise your arm straight in front of your body while standing as depicted.
- Push down with the other hand that is on top of your arm. Your arm must not be allowed to move. Try not to feel any discomfort or move the arm while you push as hard as you can.
- Maintain this posture for 30 seconds, then slowly resume your original position.
- Perform the exercise twice daily.
STRENGTHENING OF ELBOW
Method 1: Flexing the elbow
- Place your palm forward while keeping your arm straight.
- Bend the elbow as using a weight of pounds or a rubber band or piece of tubing.
- Maintain this posture for 30 seconds, then slowly resume your original position.
- Perform the exercise twice daily.

Method 2: Isometric Elbow Flexion
- Assume the position shown, placing your injured or affected arm on the bottom with the palm facing up.
- Attempt to bend the elbow of your involved/injured arm while resisting with the top hand.
- Refrain from letting your elbow budge.
- Maintain this posture for seconds before relaxing.
- Repeat the workout times each day.
Special Tests:
Provocative tests: If any of these tests are positive, there may be impingement, which could cause biceps tendinopathy. For particularly confirming or excluding biceps tendinopathy, there is currently no validated cluster of diagnostic tests available. As a result, the diagnosis should be guided by the results of these tests:
- Yergason’s test: The patient must supinate against resistance while holding his or her arm at the side with the elbow flexed at 90 degrees. When pain is sent to the bicipital groove, the test is deemed successful.
- The Neers test: It requires the arm to be internally rotated while it is flexed forward. If the patient feels pain, it may be an indication of subacromial pain syndrome or shoulder impingement syndrome.
- Hawkins Test: The patient performs the Hawkins test, flexing their elbow to 90 degrees as the doctor lifts their shoulder to 90 degrees and inserts their forearm in a neutral position. The humerus is rotated internally while being supported by the arm. If there is pain in the bicipital groove, the test is positive.
- Speeds test: The patient extends their elbow and supinates their forearm while attempting to flex their shoulder against the opposition. Radiating pain to the bicipital groove indicates a positive test result.
Arrive At Activity:
It is safe to cautiously resume regular activities or sports when the arm can be moved in all directions without experiencing any pain. Reduce activities that demand repeated lifting and overhead activity if symptoms return.
Outcome:
Biceps tendinopathy is an inflammation that can be brought on by both the aging process and a degenerative condition that typically affects athletes who perform repeated overhead movements. It’s crucial to realize that this inflammation can have a wide range of reasons, and it frequently coexists with other shoulder conditions such as instability, rotator cuff tears, or SLAP lesions.
The patient will predominantly feel pain in the bicipital groove, which may spread down to the hand or in a radial pattern toward the deltoid muscle’s insertion. causing the pain experienced during pull, push, and overhead activities to intensify.
The best technique to diagnose biceps tendinopathy is by palpating the tendon in comparison to one another along the intertubercular groove, or by doing extra-articular ultrasonography.
Conservative or surgical measures are used as treatments. If conservative therapies are ineffective after three months, surgery should be considered. The biceps tendon may need to be repaired if necessary, and structures that are the cause of primary and secondary impingement may be removed. After surgery, physiotherapy helps the most for back to activity.
FAQs:
Can I still work out with bicep tendonitis?
Rest to allow the tendon sheath to heal is therefore the most crucial biceps tendonitis treatment. However, you can exercise to maintain your shoulder and bicep mobile and your muscles strong while the injury is healing.
Can I lift weights with tendonitis?
Within a day or two of receiving the all-clear from your doctor, begin working out to strengthen the muscles surrounding the painful joint. Start with a thorough warm-up to lessen tissue stress. Then try using a flexible workout band or lifting modest weights.
What gym exercises to avoid with bicep tendonitis?
Performing pec and bicep stretches as well as actions that put the biceps in a stretch position, as well as stretching your shoulder backward, are all prohibited. Do not extend your biceps tendon while you are still recovering.
How long should I rest to heal the tendonitis?
Rest: For two to three days, try not to move the tendon. Ice: Apply an ice pack or a bag of frozen peas to the tendon for up to 20 minutes every two to three hours while wrapping it in a tea towel.
How do you rehabilitate bicep tendonitis?
Raise your damaged side arm, palms down, and touch the wall with the thumb side of your hand. Until your bicep begins to feel stretched, keep your arm straight and tilt your torso away from your lifted arm. After holding the stretch for 15 seconds, take a break and repeat the exercise twice more.