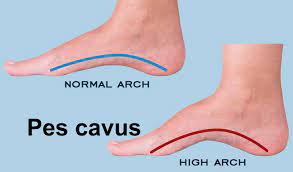
Pes cavus
Table of Contents
Definition
Pes cavus is a foot with an abnormally greater plantar longitudinal arch. Individuals who have this deformity will put too much weight and stress on the ball and heel of the foot while standing and/or walking.
The spectrum of connected deformities observed with pes cavus involves clawing of the toes, posterior hind foot deformity (described as an improved calcaneal angle), contracture of the plantar fascia, and cock-up deformity of the great toe. This may cause improved weight bearing for the metatarsal heads and connected Metatarsalgia and calluses.
Causes of Pes cavus
- The causes may be credited to the brain, spinal cord, peripheral nerves, or structural problems of the foot.
- When motor imbalance starts prior to the maturation of the skeleton, there may be a substantial change in healthy bone morphology.
- When cavus is acquired after skeletal maturity, there can be less or no change in the morphology.
- 2/3 of adults with symptomatic cavus foot have an underlying neurologic condition, most usually: Charcot-Marie-Tooth (CMT) disease, spinal dysraphism, polyneuritis, Intraspinal tumors, poliomyelitis, syringomyelia, Friedreich ataxia, cerebral palsy, and spinal cord tumors, may cause muscle imbalances that lead to elevated arches.
- A person with a new-onset unilateral deformity but without a history of trauma must be diagnosed with spinal tumors.
- The cause and deforming mechanism underlying pes cavus are too hard and not well understood.
- Factors considered influential in the development of pes cavus involve muscle weakness and imbalance in neuromuscular disease, residual effects of congenital clubfoot, post-traumatic bone malformation, contracture of the plantar fascia, and shortening of the Achilles tendon.
- Also, identify as Hereditary Motor and Sensory Neuropathy (HMSN), it is genetically heterogeneous and generally presents in the 1st 10 years of life with delayed motor milestones, distal muscle weakness, clumsiness, and frequent falls.
- Up to adulthood, Charcot-Marie-Tooth disease may cause painful foot deformities like pes cavus.
- Although it is a relatively normal disorder affecting the foot and ankle, little is identify as about the distribution of muscle weakness, severity of orthopedic deformities, or types of foot pain experienced.
- There are no particular cures or effective courses of treatment to halt the progression of any form of Charcot-Marie-Tooth disease.
- The development of the cavus foot structure seen in Charcot-Marie-Tooth disease has been priorly linked to an imbalance of muscle strength nearby the foot and ankle.
- A hypothetical model proposed by too many different authors describes a relationship whereby weak evertor muscles are overstrength by stronger invertor muscles, causing an adducted forefoot and an inverted rearfoot.
- Exactly the same, weak dorsiflexors are over-strengthen by stronger plantar flexors, causing a plantarflexed 1st metatarsal and anterior pes cavus.
- A man is a preventive factor for cave feet( pes cavus), but a risk factor for flat feet.
- There is a statistically significant difference because of sex in the prevalence of hollow feet.
Types of Pes cavus
- 3 main types of pes cavus are usually described in the literature: pes parvovirus, pes calcaneocavus, and ‘pure’ pes cavus.
- The 3 types of pes cavus may be characterized by their etiology, clinical signs, and radiological appearance.
Pes cavovarus

- The most usual type of pes cavus is seen priorly in neuromuscular disorders like Charcot-Marie-Tooth disease and, in cases of unknown etiology, is conventionally termed ‘idiopathic’.
- Pes cavovarus comes with the calcaneus in varus, the 1st metatarsal plantarflexed, and a claw-toe deformity. Radiological impression of pes cavus in Charcot-Marie-Tooth disease shows the forefoot is usually plantarflexed in relation to the rearfoot.
Pes calcaneocavus foot

- Which is looked out primarily following paralysis of the triceps surae because of poliomyelitis, the calcaneus is dorsiflexed and the forefoot is plantarflexed.
- Radiological impression of pes calcaneocavus reveals a large talocalcaneal angle.
Pes cavus
- The calcaneus is neither dorsiflexed nor in varus and is highly arched because of a plantarflexed position of the forefoot on the rear foot.
- A combination of any or all of these elements may also be seen in a ‘combined’ type of pes cavus that can be further categorized as flexible or rigid.
- Also, types of Pes Cavus is depends on the location of APEX of the deformity.
- Anterior Cavus (Forefoot Cavus) –Local –Global
- Metatarsus cavus
- Posterior Cavus
- Combined
Epidemiology
- There are few great estimates of the prevalence of pes cavus in the general population.
- While pes cavus has been reported in among two and twenty-nine percent of the adult population, there are several limitations of the prevalence data reported in these studies.
- Population-based studies recommend that the prevalence of the cavus foot is approximately ten percent.
Pathogenesis
- Too many theories have been imposed for the pathogenesis of pes cavus.
- Duchenne described intrinsic muscle imbalances causing an increased arch.
- Other theories include the extrinsic muscle and a compound of the intrinsic and extrinsic muscles being causes of the imbalance.
- Mann et al. (1992) described the pathogenesis of pes cavus in individuals with CMT disease.
- An agonist and antagonist model for the muscles describes the deformity. In CMT, the anterior tibialis muscle and the peroneus muscle generate weaknesses.
- Antagonist muscles, posterior tibialis, and peroneus longus pull stronger than the other muscles, causing deformity. Especially, the peroneus longus pulls stronger than the weak anterior tibialis causing plantar flexion of the 1st ray and forefoot valgus.
- The posterior tibialis pulls stronger than the loose peroneus brevis causing forefoot adduction.
- Intrinsic muscle creates contractures while the long extensor to the toes, recruited to assist in ankle dorsiflexion, causes cock-up or claw-toe deformity.
- With the forefoot valgus and the hindfoot varus, improved stress is put on the lateral ankle ligaments and instability may take place.
Clinically relevant Anatomy
- Clinically it is an abnormal inclination of the medial arch in weight bearing.
- Biomechanically, cavus is described as a varus hindfoot, greater calcaneal pitch, high-pitched midfoot, and plantarflexed and adducted forefoot.
- When the angle between the talus and calcaneus is short, the os navicular moves to a superior position to the cuboid, instead of medial to it.
- This makes it problematic for the Chopart-joint to function.
- The talus is the linker between the foot and the ankle. In a neutral foot, the foot rotates nearby the talus and the cuboid follows the calcaneus.
Characteristics
- At the time of the gait cycle, the foot remains locked in hindfoot inversion and forefoot varus throughout the stance phase, causing little stress dissipation.
- This may result in metatarsalgia, stress fracture of the 5th metatarsal, plantar fasciitis, medial longitudinal arch pain, iliotibial band syndrome, and instability.
- This locking and unlocking of the Chopart-joint is a crucial element in the cavus foot.
- In a cavus foot, the calcaneus is rotated inside beneath the talus, resulting in a short anterior-posterior talocalcaneal angle.
- Therefore the cuboid follows the calcaneus, the cuboid is plantar to the navicular, on the contrary beside it.
- This fixes the midfoot and surplus the lateral side of the foot.
- Another way to look at the chopart function is to look at the foot from the front with the forefoot removed.
- If an axis, drawn through the 2 joints, is parallel to the ground, there will be relatively free flexion.
- The more the axis approaches a vertical orientation, the little flexion will be possible.
- In extremely high-arched feet, the weight bearing is distributed roughly along the metatarsal heads and the lateral border of the feet.
- This kind of disorder causes the foot to prone to metatarsal head and calcaneal contusions, originating from too much pressure of weight bearing.
- Also, the foot is prone to osteophyte formation at the intersection of the metatarsal bases and the cuneiforms.
Symptoms of Pes cavus
People complain of pain, instability, difficulty walking, and problems with footwear. The symptoms differ with the degree of deformity .and also may present with lateral foot pain from improved weight bearing on the lateral foot. The range of complaints reported in the literature involves metatarsalgia, pain underneath the 1st metatarsal, plantar fasciitis, painful callosities, ankle arthritis, and Achilles tendonitis:
- Keratosis
- Lateral Ankle instability
- Hindfoot varus
- The forefoot plantar flexion
- Hindfoot varus
- Lower limb stress fractures
- Knee pain
- Iliotibial band friction syndrome
- Back pain
- Tripping
Clinical Tests
- The Coleman block test identifies if the subtalar joint is flexible.
- The test is done by having a patient stand with a one-inch wood block underneath the heel and lateral foot.
- This permit the 1st ray to be plantar-flexed off the block.
- If the hindfoot is accurate to a neutral position, the deformity is flexible.
- If the hindfoot does not correct at the proper time, the deformity becomes rigid.
- Increased calcaneal angle.
Medical Treatment
- Medical management is to permit the patient to ambulate without any problems.
- It is necessary for the patient to understand that surgical reconstruction does not give a normal foot.
- The main focus of surgical reconstruction is to generate a plantigrade foot and pain relief.
- Repeated surgical procedures may be important, specifically if the deformity is progressive.
- Surgical procedures may be largely categorized into soft-tissue and bony procedures.
- Tendon transfers and osteotomies may give correction of the deformity without requiring an arthrodesis.
Physiotherapy Treatment in Pes cavus
- Recommended conservative management of people with painful pes cavus usually includes strategies to decrease and redistribute plantar pressure loading, with the use of foot orthoses and specialized cushioned footwear.
- The orthoses for pes cavus require to accomplish several specific goals:
- Enlarging plantar surface contact area.
- The overload on the metatarsal heads is a result of restricted plantar surface contact because of high arch and limited ankle joint dorsiflexion. Increasing the plantar surface contact make certain the foot bears more weight in the arch while the metatarsal heads bear little weight during activity.
- Resisting against excessive supination.
- Lateral ankle stability and laterally deviated subtalar joint axis (STJ) are often connected with high-arched feet.
- This position outcome in too much supinator torque around the subtalar joint axis.
- Resisting against inactive pronation and supination forces Rearfoot instability is caused by an extension of the laterally deviated subtalar axis.
- In flexible pes cavus, midtarsal flexibility mixes up the later portion of the stance phase of gait.
- The forefoot pathology generates midtarsal joint supination, which leads to extra pronation of the rearfoot.
- Some pes cavus people hurt from pair of lateral ankle instability at midstance and rearfoot pronation at later midstance.
- Stretching and strengthening of tight and weak muscles, debridement of plantar callosities, osseous mobilization, massage, chiropractic manipulation of the foot and ankle, and strategies to improve balance.
- Orthotics with some extra-depth shoes to offload bony prominences and prevent rubbing of the toes can increase symptoms.
- For varus deformities, a lateral wedge sole modification may increase function.
- Bracing for supple deformities or foot drop can permit the person to ambulate; however, in patients with sensation deficits, Plastazote linings in the brace are needed and often inspection of the skin for ulceration is warranted.
Surgical Management
- Correcting a cavovarus foot
- Most of the corrections include tendon transfers and capsular and facial releases
- Correction of plantar flexion of the 1st ray by performing a dorsiflexion
- ST tarso-metatarsal arthrodesis.
- Declination of hindfoot varus by performing a lateralizing calcaneal osteotomy.
- Arthrodesis 1st TMT joint, lateral calcaneal osteotomy for hind foot.
FAQ
The spectrum of connected deformities observed with pes cavus involves clawing of the toes, posterior hindfoot deformity (described as an improved calcaneal angle), contracture of the plantar fascia, and cockup deformity of the great toe.
Static neurological disorders that cause cavus foot involve stroke, polio, cerebral palsy, spinal injury, and peroneal nerve injury. Progressive neurological disorders that may cause cavus foot involve a spinal tumor, brain tumor, spinal cyst, muscular dystrophy, Friedreich’s ataxia, and Charcot-Marie-Tooth syndrome.
Pes cavus is afoot with an abnormally greater plantar longitudinal arch. Individuals who have this condition will put too much weight and stress on the ball and heel of the foot at the time of standing and/or walking.
Cases of cavus foot caused by a neurological disorder are likely to worsen over a period of time, but cavus foot will likely remain the same when caused by a medical condition or inheritance. Cavus’s foot will cause pain when walking, specifically over long periods.
There are studies that have ruled that walking barefoot may make arches stronger and higher. Underused muscles and ligaments are activated. Feet are in their ordinary position and there is nothing to restrict the full range of motion. This natural movement can help to strengthen the arches.