

Madelung’s Deformity of the wrist
Table of Contents
Description
Madelung’s deformity is an abnormality of the palmer ulnar part of the distal radial epiphysis in which progressive ulnar and volar tilt develops at the distal ulna. First described by Bt Malgaigne in 1855 and later by Madelung in 1878.
Though congenital, it is obvious until late childhood and adolescence. It is a rare condition, with an incidence being only 1.7 percent. A Vickers’ ligament is the feature to identify Madelung’s deformity from Madelung-like deformities.
Epidemiology
- Predominantly adolescent women are affected by a ratio of 4:1.
- The deformity is bilateral most frequently.
Symptoms of Madelung’s Deformity
- Initially asymptomatic, progressive clinical deformity.
- Pain at the wrist.
- Loss of wrist extension.
- Compromised forearm rotation.
- “Bayonet” deformity- prominent distal ulna as an outcome of dorsal subluxation.
- Girls are more often affected than boys.
- Mostly happen between the ages of 6 and 13 years.
Pathogenesis
- Premature growth plate seizes at the medial volar aspect of the distal radius be the cause of Madelung deformity.
- Continues traumatic pressure can result in Madelung-like deformity.
- Mutation or absence of the short-stature homeobox (SHOX) gene is believed to be the cause of congenital Madelung deformity.
- Congenital Madelung deformity may take place as a part of Leri-Weill dyschondrosteosis (LWD) or Turner syndrome.
Diagnosis
X-ray

- Key Features from X-Ray.
- Improved dorsal and radial convexity of the distal radius.
- Improvement of volar and ulnar tilt of the distal radial articular surface.
- Widened interosseous space.
- Relative dorsal position of the ulnar head.
- Pyramiding of the carpus.
MRI
- MRI is done on patients who require the surgical release of Vickers’ ligament to prevent deformity progression.
Differential Diagnosis
- Turner syndrome
- Nail-patella syndrome
- Hereditary, multiple exostoses
- Ollier’s disease
- Achondroplasia
- Multiple epiphyseal dysplasias
- Mucopolysaccharidoses (Hurler and Morquio syndrome)
Treatment of Madelung’s Deformity
Medical management-
- oral analgesics
- activity restriction
- volar splint
Physiotherapy treatment
To reduce pain
- Icing
- Hot Cold whirlpool bath immersion
- Transcutaneous electrical nerve stimulation (TENS)
To improve range of motion
Palms to the sky/Palms to the floor
- This gentle exercise provides a tiny stretch to the wrists while generating strength.
- While sitting or standing, hold the arms out in a T position.
- Rotate hands so palms are facing up.
- Rotate hands so palms are facing down.
- Do it a further ten times.
- Try to keep up the shoulders and neck relaxed.
- The movement should be just in the wrists, not the arms, elbows, or shoulders.
Fist to jazz hand
- This is another simple exercise that mainly focuses on hand flexibility and strength.
- Rest one arm on a table, like the patient is about to arm-wrestle someone.
- Make a fist.
- Gently open the fist and stretch the fingers out as wide as they can comfortably go (do a jazz hand).
- Do it further 10 times, then switch arms.
- Singing “All That Jazz” is optional.
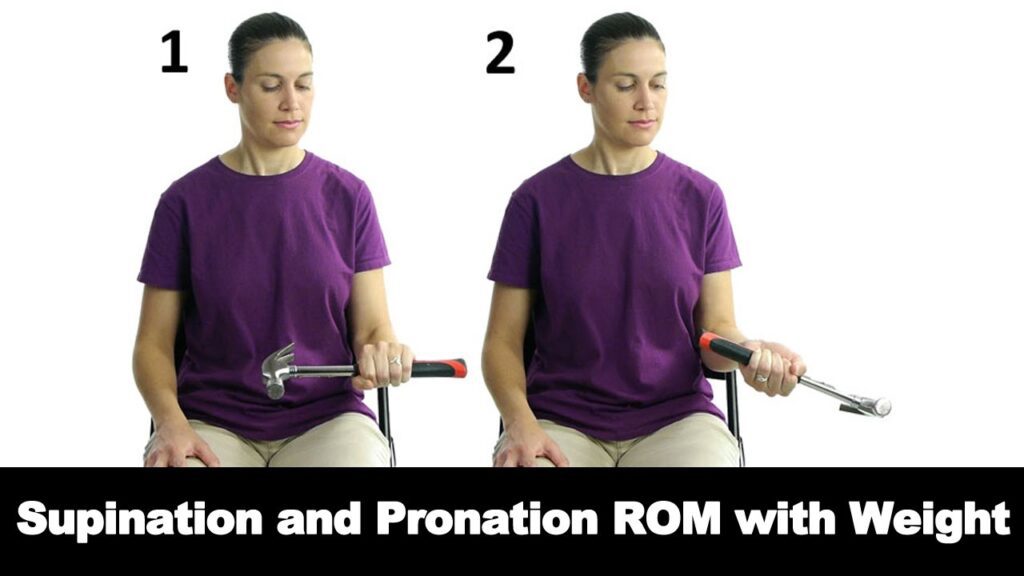
Rotation

- The patient may do this with no weights.
- Begin with no weights and add weight only if the person feels no pain.
- Sit with the arms bent to 90 degrees and forearms out in front of you with palms facing down.
- Hold a light resistance band or dumbbells, or go weight-free and pretend that holding something.
- Gently rotate the hands so the palms are facing up.
- Gently rotate the palms back to the starting position.
- Do it a further 10 times.
Wrist curl
A person can perform this movement with a resistance band, a dumbbell, or just bodily resistance. If the person is using a light resistance band, hold one end of the band down with the bottom of the foot and grab the other end with the working hand. For dumbbells, initially try with 1–5 pounds, depending on the patient’s level.

- Start with sitting on a comfortable chair sit and hold the arm at 90 degrees, with the palm facing up.
- The arm may rest on the leg, a bench, or a table.
- Bend the wrist up, like it is doing a baby biceps curl.
- Return the wrist to the starting position.
- Do it 10 times, then switch sides.
- Make sure to move only the wrist.
- It is not a biceps curl, it is a wrist curl, so keep the arm and shoulder still while the wrist does all the work.
Pronated wrist curl
- These are pretty much upside-down wrist curls.
- The patient may use a dumbbell, a band, or nothing at all.
- Sit and hold the arm at 90 degrees, with the palm facing down.
- Curl the wrist up. Return the wrist to the starting position.
- Do it for10 times, then switch sides.
- As with the previous move, be sure the movement is only in the wrist.
- The person may want to position the arm so the wrist may hang off the leg or a bench.
- If the wrist starts by hanging down about 90 degrees, the person will get a better range of motion for the exercise.
Squeeze
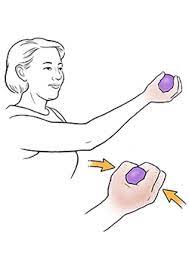
- The patient may squeeze just about anything in this one.
- Do with using a tennis ball, hand grip exerciser, or towel.
- While standing or sitting, hold the ball (or squeezable thing of choice) with the palm facing up.
- Squeeze the squeezy thing as hard as a person may for 3 to 4 seconds.
- Gently release the grip.
- Do it 10 times, then switch sides.
Wrist extension

- Maintain the right arm straight out in front of you, With the left hand, gently pull your right hand back until the person feels a stretch in the right forearm.
- Hold for 15 seconds, then switch arms.
- Repeat further the sequence 5 to 6 times.
- Be gentle, the patient does not need to pull anything, so go gently and do not force any movements.
Wrist flexion
- This is the opposite of the last stretch.
- Just hold the right hand down with the wrist at 90 degrees.
- With the left hand, gently press the right hand back toward the body until the person feels a stretch across the back of the right hand and wrist.
- Hold for fifteen to twenty seconds, then switch arms.
- Do it further 5 times.
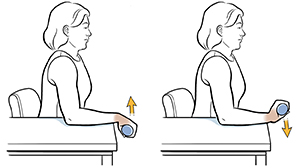
Wrist Supination With Dumbbell
- Sit in a chair with the side of the forearm resting on the table and the wrist and hand hanging over the edge.
- The thumb should face the ceiling.
- Hold the edge of a small (1- to 3-pound) dumbbell in the hand, like you would hold a hammer.
- Gently permit the hand and wrist to rotate over so the palm is facing up toward the ceiling.
- Hold the end position for a few seconds, then slowly rotate the hand back up, so the dumbbell is straight up once again.
- The patient may merge the supination exercise with the pronation exercise explained in the next step, alternating which way you rotate the wrist.
Wrist Pronation With Dumbbell
- Wrist pronation refers to the position of the hand facing down as if you were pouring a pitcher of water.
- To strengthen the wrist pronators, sit in a chair with the forearm supported on a table and your wrist and hand over the edge.
- Hold one edge of a dumbbell with the weight pointing up towards the ceiling.
- Gently rotate the hand, so your wrist and palm are facing down towards the floor.
- Hold this position for a few seconds, then gently turn the hand back to the starting position with the weight pointing up towards the ceiling.
- Do two to three sets of 10 to 15 repetitions.
Namaste stretch

- Press the palms together in a Namaste pose right under the chin, with elbows out to the sides.
- Lower hands toward the belly button, keeping up the palms stuck together.
- When the person feels a stretch, hold it there for thirty seconds.
- Do it further for 2–4 more times, whatever feels good.
Surgical Management
For pediatrics
- Physiolysis
- Dome osteotomy
- Vickers Ligament Release
For adults
- Ulna reduction
- Total DRUJ replacement
- Dome Osteotomy
FAQ
Madelung’s deformity is a deformity of the wrist where part of the distal radius does not grow properly, leading to subluxation (partial dislocation) of the wrist bones between the radius and ulna. The distal joint between the radius and ulna is dislocated, majoring to a prominent bump from the head of the ulna.
All cases of Madelung’s deformity are thought to have a hereditary component; although, the genetic origins are compound and our understanding is evolving. Madelung’s deformity is known to be connected with different skeletal dysplasias and syndromes.
Madelung deformity may be bilateral in 50-66% of patients. It frequently occurs as a rare congenital deformity and does not normally manifest until 10-14 years of age. It can also be seen as an acquired consequence of trauma to the growth plate, For example, Salter-Harris fracture (type V).
With osteoarthritis, the cartilage starts to wear away over time. In some cases, the cartilage may fully wear away, leaving nothing to protect the bones in a joint, causing bone-on-bone contact. Bones can also bulge, or stick out at the end of a joint, called a bone spur.
Pseudo-Madelung deformity refers to improved radial inclination (i.e. ulnar tilt) of the distal radius but with negative ulnar
variance and the absence of some other typical features of Madelung deformity.




2 Comments