
Hip Bone
Table of Contents
Introduction
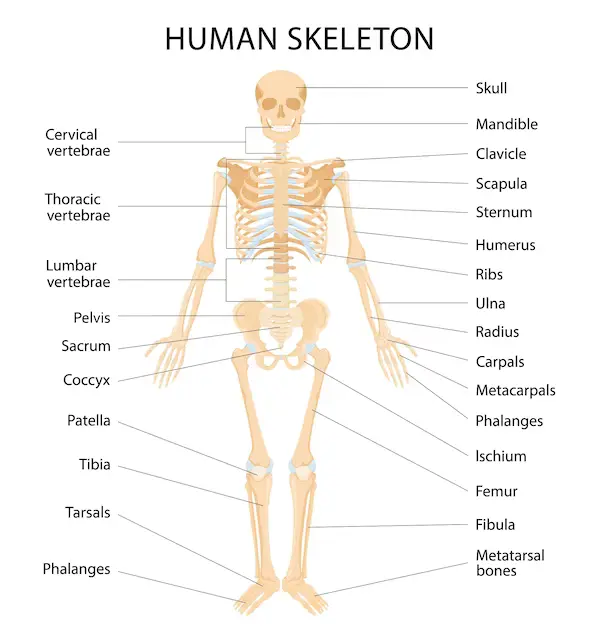
The hip bone, also known as the coxal bone or innominate bone, is a large, flat bone that forms the pelvis, which is the bony structure that supports the torso and connects the lower limbs to the body. The hip bone consists of three fused parts: the ilium, the ischium, and the pubis. The ilium is the largest of the three parts and forms the superior aspect of the hip bone, while the ischium forms the posterior and inferior aspect, and the pubis forms the anterior aspect. Together, these three parts form a cup-shaped socket called the acetabulum, which articulates with the head of the femur to form the hip joint.
The hip joint is the connection where the hip attaches the leg to the body’s storage area. It’s made up of two bones: the pelvis, which is made up of the ilium, ischium, and pubis, and the femur, which is the thighbone. The hip joint’s ball is made by the femoral pioneer, while the attachment is made by the hip bone socket.
The pelvis bones are a necessary part of the major parts of the structure. They work as a difference between the axial structure and the appendicular structure of the lower body, serving as an attachment point for some of the numerous powerful muscles in the human body while fighting the forces generated by them. The curved surface of the pelvic bone completes a secured network, itself lined with different muscles and housing different blood supplies, lymphatic structures, nerves, and organs, including the intestines, urinary bladder, and internal coupling organs.
The pelvic support, or innominate bones, is the hard system that interfaces the pivotal skeleton to the lower appendages. Both the left and right hip bones have different shapes.
Structure and Function

The pelvis is included the huge hip bone, the os coxae, on an alternate side. The os coxae itself is made out of the ilium (the level unrivalled bulge), ischium (the bent front projection), and pubis bones (the bent substandard projection). The os coxae append anteriorly to each other at the pubic symphysis and posteriorly to the novel side of the sacrum, shaping the sacroiliac joint. These three os coxae bones total each other at the hip bone socket, an average construction that fills in as a connection pinpoints for the top of the femur. The pubis and ischium even lucid poorly at the ramal epiphyses, with their bending nature leaving a presentation between them known as the obturator foramen. This foramen permits the obturator nerve to leave the pelvic opening.
Each of the pelvic bones again has many landmarks (i.e., tuberosities, notches) individual to the detailed bone. The superior border of the ilium is called the crest of the ilium, or, more formally, the iliac crest, with a tuberosity below it on the ilium’s anterior edge is understood as the anterior inferior iliac spine. The ileum also has a posterior-inferior landmark understood as the greater sciatic aperture on it, with a following lesser sciatic not living on the posterior-inferior side of the ischium. On the anterior side of the exact boundary of the ischium is the tuberosity of the ischium.
The primary position of the pelvic bones is to communicate the hurdle of the upper body onto the lower limbs while standing or walking. This part occurs via the connection of the axial and appendicular structures at the sacroiliac joint. When a man stands exemplary, the centre of gravity lies in the body’s centre. The pelvis sends the load to the femur and both lower furthest points. The severe form of these bones again covers the organs that lie within their captivity. Such organs contain The bladder, rectum, urethra, and uterus in women.
The hip bones have three main articulations:
Sacroiliac joint – articulation with the sacrum.
Pubic symphysis – expression between the left and proper hip bones.
Hip joint – sign with the top of the femur. The hip bones’ anatomy, including their arrangement, bony landmarks, and clinical applicability, will be examined in this report.
Arrangement of the Hip Bone

There are three parts to the hip bone: the pubis, ischium, and ilium. These parts are split by the triradiate cartilage before puberty, and fusion only begins between the ages of 15 and 17. The acetabulum—which translates to “vinegar cup” in Latin—is a cup-shaped socket that is present in the ilium, pubis, and ischium concurrently. The hip joint is formed when the charge of the femur and the acetabulum communicate. We will take a close look at the various hip bone components and their bony landmarks.
The Ilium
The ileum is the absolute most complete and biggest of the three pieces of the hip bone and is found superiorly. The body of the ilium shapes the unrivalled piece of the hip bone socket (acetabular rooftop). Straight over the hip bone socket, the ilium reaches out to incorporate the wing (or all).
The branch of the ilium includes two surfaces:
Inner surface – has an indented form, which delivers the iliac fossa (site of origin of the iliacus muscle).
Exterior surface (gluteal surface) – has a convex profile and provides attachments to the gluteal muscles.
The most significant margin of the wing is focused, forming the iliac crest. It damages the anterior superior iliac crest (ASIS) to the posterior superior iliac spine (PSIS). On the posterior part of the ileum, there is an indentation understood as the more prominent sciatic notch.
The Pubis
The pubis is the multiple anterior parts of the hip bone. It consists of a body, a most prominent ramus, and a low ramus (ramus = branch).
Pubic body – found medially, it conveys with the inverse pubic body at the pubic symphysis. Its most noteworthy component is set apart by a round thickening (the pubic peak), which opens horizontally as the pubic tubercle.
Special pubic ramus – spreads laterally from the body to create part of the acetabulum.
Nether pubic ramus – tasks towards the ischium. Concurrently, the greatest and inferior rami hold part of the obturator foramen – via which the obturator nerve, artery, and vein parts contact the lower limb.
The Ischium
The hip bone’s posteroinferior aspect is included in the ischium. It has a body, an inferior ramus, and a superior ramus, much like the pubis. The ischiopubic ramus, which contains a portion of the obturator foramen, converges with the inferior ischial ramus and the inferior pubic ramus. The ischial tuberosities are formed by the posteroinferior portion of the ischium, and when posing, our body’s importance is placed on these tuberosities. A posteromedial projection revolves around the point where the largest ramus and body meet.
Embryology
Pelvic bones form their development as mesenchymal tissue of the embryonic more inferior limb buds. This mesenchyme forms spreading out in three movements, coordinating with each of the three bones of the os coxae. The ischial and pubic masses relocate around the obturator nerve, uniting inferiorly to form the obturator foramen. Each pubic group migrates medially to meet at the future pubic symphysis, while interactions with the primitive spinal cue draw the iliac mass toward the sacrum derived from notochord mesenchyme. These mesenchymal assemblies then experience endochondral ossification, with ilium, ischium, and pubis including primary ossification at the third, fourth-to-fifth, and fifth-to-sixth months of pregnancy, respectively. The future acetabulum lies close to each bone’s primary site of ossification, with each bone’s ossification function fanning out superiorly, inferiorly, and anteriorly. Sacral ossification starts in the third month, with a piece of the vertebrae having three centres of ossification. Secondary ossification appears during the first year of life. Secondary ossification posts are at the manifestation of the three pelvic bones in the acetabulum, the spine of the ilium, anterior inferior iliac divide, tuberosity of the ischium, symphysis pubis, and Ramal epiphyses. These change plates are complete during mid-puberty.
Blood Supply and Lymphatics
Many blood containers are included within the crater formed by the pelvic bones. These plates contain the typical iliac artery, external and internal iliac artery, superior and subordinate gluteal artery, obturator artery, greatest vesical route, and interior pudendal artery, along with its coincident veins. Some of these routes and their components, such as the internal iliac, stay within the pelvic hollow while others transit out, such as the gluteals and outer iliac, to deliver features such as the buttocks and more inferior limbs, respectively. The gonadal and uterine routes will also run across and into the pelvic cavity, respectively, counting on sex. Major lymph nodes in this province contain the obturator, everyday iliac, external and internal iliac, hypogastric, superior rectal, presacral, presacral, promontory, or perirectal nodes. Nodes with the corresponding vasculature occur in pairs, one being on the anatomical left and the different on the anatomical right. Pelvic lymph nodes are a common area of prostatic and gynecologic cancer metastasis.
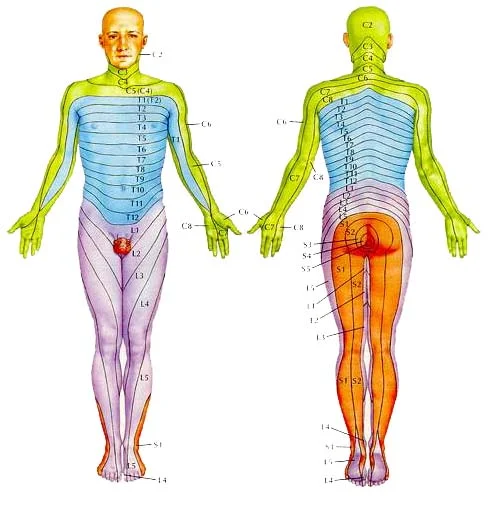
Nerves
The pelvic bones, and the girdle created by them, house nerves from the lumbar and sacral plexuses. Nerves of the lumbar plexus contained in the pelvis from the genitofemoral, lateral femoral cutaneous, obturator, and femoral nerves. The genitofemoral spears via the psoas muscle posterior-to-anterior to contact the genital region on the anterior face of the pelvis. The lateral femoral cutaneous nerve departs the crest and transverses the pelvis going under the anterior brim of the crest of the ilium to contact the thigh. The obturator nerve dives medially to the psoas to exit the pelvis via the obturator foramen. The femoral nerve varies between the psoas and the iliacus, appearing from the pelvis further to the pubis to continue into the anterior thigh. Sacral plexus nerves of the pelvis form the sciatic, superior, and inferior gluteal, posterior femoral, and pudendal nerves. The first four of these nerves all exit the pelvis crossing under the greater sciatic notch, serving innervations on the posterior gluteal and thigh areas. The superior gluteal nerve provides innervations to the gluteus minimus and medius, while the low gluteal innervates the gluteus maximus, which extends the hip. The pudendal nerve crosses within the pelvic girdle, sending interventions to various sphincters and genitalia formats. This nerve generally gets injured during the vaginal delivery of children.
Muscles
The muscles of the pelvis are essential in possessing the power of the pelvic girdle, holding a standing posture, and supporting the movement of the crate and lower extremities. The interior iliac crest serves as the origin of the Iliacus muscle, which crosses inferiorly and completes with the psoas, which are requirements above the pelvis but travels down via it, to make the iliopsoas. This muscle finally exits the pelvis and inserts itself upon the femur. The piriformis is another force that creates inside the pelvis and inserts externally on the femur.
The pubic symphysis processes as an attachment point for both abdominal muscles, including the rectus abdominis, internal and external obliques, and transversus abdominis, as well as muscles of the adductor chest of the leg, involve the adductor brevis/longus/Magnus, gracilis, and pectineus. United along the nether edges of the pubis bearing posteriorly to the sacrum are the pelvic floor muscles, which contain the puborectalis, iliococcygeal, iliococcygeus, pubococcygeus, external anal sphincter muscles, and levator ani. The obturator internus muscles even have insertions on the internal side of the pubis and traverse on the pelvic floor muscles, eventually leaving the greater sciatic notch and inserting it on the behind surface of the femur. The obturator externus travels from the anterior front of the pubis posteriorly to insert on the backside of the femur as well. The gluteal muscles, quadratus femoris, and semitendinosus muscles all even maintain branches on the pelvic bones. The inguinal ligament, a common anatomical landmark applied with a hernia, runs from the anterior part of the iliac spine to the front of the pubic symphysis.
Ligaments
The ligaments of the hip joint can be separated into two groups; capsular ligaments and intracapsular ligaments. Capsular ligaments are born ligaments of the joint capsule. 3 capsular ligaments play a fundamental role in possessing the goodness of the joint during various motions: iliofemoral, pubofemoral, and ischiofemoral ligaments. The intracapsular ligaments of the hip joint are found inside the capsule and hold the transverse ligament of the acetabulum and the ligament of the leader of the femur.
Iliofemoral ligament
Synonyms: Y-ligament of Bigelow, Ligament of Bertin
The iliofemoral ligament is a thick triangular ligament that lies on the anterior and superior portions of the hip joint and blends with the joint capsule. Its proximal attachment is between the anterior inferior iliac spine and the acetabular frame. Distally, it communes to the intertrochanteric line. The prominent part of this ligament is more delicate and reached with its extreme bands, giving the ligament an inverted Y-shape. It is the most effective ligament in the body and positions to prevent hyperextension of the hip joint when standing.
During augmentation, this tendon tenses, contracting the case and associating the femoral head firmly to the hip bone socket. This activity decides the connection of the hip joint past the upward position to between 10o to 20o.
Pubofemoral ligament
The pubofemoral tendon untruths anteroinferior and helps the foremost and mediocre pieces of the joint container. It appears from the ischiopubic ramus, the superior pubic ramus, and the obturator crest of the pubic bone. It heads out along the side and poorly to the lower section of the intertrochanteric line, talking with the stringy layer of the joint container and the average band of the iliofemoral tendon.
The lightest pieces of the joint container are between the average strings of the iliofemoral and the pubofemoral tendons where there is a roundabout indent. The tendon of the Iliopsoas muscle overlaps this area. Between the muscles tendon and the tablet is the iliopectineal (psoas) bars which correspond with the hip joint cavity. The pubofemoral ligament includes excessive abduction of the hip joint by removing during extension and abduction movements.
Ischiofemoral ligament
Synonyms: ischiocapsular ligament, Ligamentum ischiocapsulare
The ischiofemoral ligament is the most helpless of all the 3 capsular ligaments. It lies posteriorly and supports the posterior aspect of the joint capsule. It is concatenated medially to the ischial bone below the acetabulum. It drives superolateral around the capsule and rear to the femoral neck to attach to the ground of the greater trochanter, profound to the iliofemoral ligament. Some of the deeper fibres of the ischiofemoral ligament combine with the zona orbicularis.
Transverse ligament of the acetabulum
The acetabular foramen, through which neurovascular structures enter the hip joint, is formed by the strong, flat transverse ligament of the acetabulum, which connects the acetabular notch to the acetabulum. It connects the acetabular labrum in the periphery and fills in the acetabular edging’s inferior gap.
Ligament of the head of the femur
This ligament is a flattened triangular band of connective tissue that has no significant contribution to the power and stability of the hip joint. Its bottom connects to the acetabular notch and the transverse acetabular ligament, while its apex connects to the fovea capitis. It contains a small portion of the obturator artery, which is the artery to the head of the femur and contributes to the blood collection of the femoral head. It is surrounded by a synovial membrane.
Physiologic Variants
The pelvis in females is very different from that of males; this is very meaningful for females to deliver an acceptable birth canal for the large head of the fetus during birth. To complete these means, the female pelvis is commonly broader and shallower (gynaecoid shape). The birth channel has to be rounded and more spacious. The sciatic notch is much more exhaustive with shorter symphysis pubis, and the pubic bones have a broadly broader angle than each other. The female coccyx is better mobile, and the sacrum is shorter and less curved.
Movements
Movements Thigh abduction Femoris abduction Synonyms: Standing as a ball-and-socket joint, the hip joint accesses in three degrees of freedom: abduction coxae circumduction, external rotation, internal rotation, flexion, extension, abduction, and adduction.
The thigh is pulled toward the chest when the hip joint is flexed. The hip joint can be flexed when the knee is bent, bringing the thigh closer to the anterior abdominal wall. Inactive flexion has a movement range of about 120 degrees, while functional flexion has a movement range of about 145 degrees. The tension in the hamstrings when the knee is extended indicates hip flexion.
The thigh is pushed away from the trunk when the hip joint is extended. The shape of the articular surfaces and the tension of the capsular ligaments restrict joint extension above standing to about 30 degrees.
Abduction and adduction of the surface of the hip joint in the coronal plane have a free range of motion of approximately 45 degrees. The range of abduction is significantly greater when the hip is flexed than when the hip is extended. Tightness in the adductor muscles and pubofemoral ligaments prevents hip joint abduction. Additionally, hip flexion makes adduction more comfortable. Contrarily, adduction is determined by the opposing limb, muscle tension in the abductor, the lateral aspect of the iliofemoral ligament, and the thigh fascia lata.
In contrast to the long hub of the femoral shaft, the surfaces of the hip joint rotate inwardly and outwardly in a plane around the mechanical hub of the femur. The mechanical hub contrasts with the intercondylar indent of the distal femur on the femur’s top. The femoral shaft pushes anteriorly during the inside pivot, initiating the toes at a medial point. The femoral shaft moves posteriorly during the outer turn, moving the toes to the point where they are missing from the midline, revealing the inversion. The outside turn is freer and has more power than the inside revolution. For instance, when the hip is extended, the inside revolution takes about 35 degrees, while the outer turn takes about 45 degrees. Hip flexion, as opposed to expansion, typically allows for much more freedom of movement when turning at the hip joint. Coziness in the equal rotators and the ischiofemoral ligament cut off
Muscles acting on the hip joint
There are functional groups for the major muscles in the hip that are responsible for the actions of the joint; lateral and medial rotators, as well as flexors, extensors, adductors, and abductors Under two active groups, a single muscle may contract. Numerous muscle information in both flexion and adduction as well as kidnapping and inner pivot.
Flexion – Psoas major, iliacus, and rectus femoris; helped by pectineus, tensor fasciae latae, and sartorius
Extension – Gluteus maximus, biceps femoris, semitendinosus,
the semimembranosus and adductor magnus
Abduction – Glutei medius and minimus; helped by tensor fasciae latae, piriformis, and sartorius
Adduction – Adductors longus, gracilis brevis and magnus; assisted by pectineus, quadratus femoris and the inferior fibres of gluteus maximus
Internal rotation Glutei minimus and medius; helped by tensor fasciae latae and most adductor muscles
External rotation – Gluteus Maximus, obturator externus and sartorius,obturator internus, superior and inferior gemelli, assisted by quadratus femoris
Mnemonic: Patched Goods Usually Go On Quilts (PGOGOQ)
(Gemellus superior, Obturator internus, Gemellus inferior, piriformis, Obturator externus, Quadratus femoris )
The iliopsoas muscles (psoas major and iliacus) and the rectus femoris muscle are the primary flexors of the hip joint. The tensor fasciae latae of the pectineus and sartorius muscles serve as weak flexors. Again, in addition to their adductor function, the adductor longus and brevis can assist with hip flexion.
The gluteus maximus muscle serves as the hip joint’s primary extensor, with help from the adductor magnus muscle and the hamstring muscles (semitendinosus, biceps femoris, and semimembranosus). and gluteus medius The gluteus minimus muscles are the hip joint’s primary abductors. Hip abduction is also helped by the muscles in the sartorius, piriformis, and tensor fasciae latae. The hip abductors reproduce a utilitarian capability in balancing out the pelvis during normal periods of the stride cycle.
The adductors longus, brevis, magnus, and gracilis muscles are the major adductors of the hip joint. The pectineus, quadratus femoris, and gluteus Maximus inferior fibres aid in these.
The front strands of the glutei minimus and medius are the chief muscles solid for the interior turn of the hip joint. The majority of the adductor muscles and the tensor fasciae latae provide support for these muscles.
The gluteus maximus and a group of six small muscles known as the lateral rotators work together to produce external rotation: quadratus femoris, obturator externus, superior and inferior gemelli, and piriformis.
Clinical importance
A deficiency of muscles of the pelvis, such as in limb-girdle muscular dystrophy, will result in an irregular waddling type of gait. A unilateral deficiency of the hip abductor muscles or subluxation of a hip joint will drive a Trendelenburg gait. An analysis of how a patient’s steps can give indications of the underlying problems related to the structure and position of the pelvis.
Surgeries completed on pelvic structures may be problematized by excessive bleeding or hematoma formation. The medical procedure may likewise be muddled by disease and sore development. In the pelvis, a hematoma or spot usually remains localized in the retroperitoneal region just in front of the iliopsoas muscles. The production is often related to the reduction of the femoral plexus or the femoral nerve in the retroperitoneal space. The patient will present with postoperative deficiency of the hip flexors and knee extensors with or without the involvement of the obturator muscles, leaning on whether it is the reduction of the femoral plexus or the femoral nerve. A female with a male class (android) of the pelvis will encounter problems during childbirth, which is one of the most dominant indications for a caesarian section.
Clinical importance – Anterior Superior Iliac Spine
The anterior superior iliac spine (ASIS) is a significant anatomical landmark: The mid-inguinal point – halfway between the ASIS and the centre of the pubic symphysis. The femoral route can be palpated here. Mid-point of the inguinal ligament – centre between the ASIS and the pubic tubercle. In clinical preparation, a patient’s “true” leg length is calculated from the ASIS to the medial malleolus at the ankle joint. This is distinct from “apparent” leg length, which is calculated from the umbilicus to the medial malleolus. True leg length difference is a feature of various hip conditions, as well as standing a potential difficulty of hip joint replacement (arthroplasty).
Clinical importance – Pubic Rami Fractures
Pubic rami fractures can occasionally be observed on x-rays in geriatric patients who are examined after simple low-energy falls from standing height. In this context and delivered they are the only damage a patient has sustained, these fractures are usually treated without surgery. Recovery can be expected within 6-8 weeks and patients are prompted to fully weight bear straightaway.
Clinical importance – Pelvic Fractures
There are 2 general groups of pelvic fractures: Low energy injuries: For example, a simple fall from standing height in an osteoporotic patient resulted in a pubic rami fracture. These are usually ‘regular’ injuries, not demanding surgery.
High power injuries with direct or transmitted trauma: For example, after a high-speed road traffic accident. These result in better extensive fractures which may contain the acetabulum and sacroiliac joint. These can be ‘unstable’ injuries and may demand urgent surgery. Higher power injuries can be associated with smooth tissue and vascular injury. In individuals, the bladder and urethra live at high risk of damage. Vascular injury can result in life-threatening haemorrhage. In the context of a high-energy primary trauma patient, the pelvis can be a prominent start of bleeding due to fracture. As a result, major trauma patients are supposed to have a pelvic fracture until proven otherwise, and a ‘pelvic binder’ is used to stabilize the pelvis and minimize other bleeding. Circumferential pressure is applied by the binder at the class of the greater trochanters – an
important anatomical landmark.
FAQ
femur
The thigh bone or femur and the pelvis join to begin the hip joint.
The hip joint is named the (ball and socket) joint. The “ball” is understood anatomically as the femoral head; the
“socket” is part of the pelvis understood as the acetabulum.
Most of the arteries of the hip area arise from the external iliac artery and include the Femoral artery. Superficial circumflex
iliac artery. External pudendal artery.
Muscles and Tendons of the Hip Joint
There are 3 muscles (gluteus minimus, gluteus maximus, and gluteus medius) that connect to the back of the pelvis and insert
into the greater trochanter of the femur.
Articular surfaces
The acetabulum is created by the fusion of the ilium, ischium, and pubic bones. It plays an important role in the stability of the hip
joint as it nearly entirely encompasses the head of the femur.


One Comment