Elbow mobilization exercise
Table of Contents
What is mobilization for the elbow joint?
- Elbow Mobilization is a passive, skilled, manual therapy technique applied to joints and related to the soft tissue at various speeds and amplitudes using physiological or accessory movement for therapeutic purposes
- small amplitude force applies at a fast velocity, and a large amplitude force applies at a slow velocity
- it is a manual technique that includes appealing to the target forces on a painful, stiff or otherwise negotiated jointly concerning improving its overall function. Which is not convenient in all situations, joint mobilizations help improve the range of motion, reduce pain, and minimize stiffness.
- Elbow Joint mobilization is a hands-on treatment that is frequently executed by physical therapists healthcare professionals who specialize in rehabilitation for movement disorders and chiropractors, health professionals treating disorders of the musculoskeletal system that involve bones, muscles, and soft tissue
Introduction for elbow joint

there are 4 joints in the elbow complex for mobilization of the elbow joint
- humeroulnar joint
- humeroradial joint
- proximal radioulnar joint
- distal radioulnar joint
Humeroulnar joint
- The humeroulnar joint also called the ulnohumeral or trochlear joint is part of the elbow joint. It is composed of two bones, the humerus, and ulna, and is the junction between the trochlear notch of the ulna and the trochlea of the humerus. It is classified as a simple hinge-joint variety, which grants movements of flexion, extension, and circumduction. attributable to the obliquity of the trochlea of the humerus
- When the forearm is extended and supinated, the axis of the arm and forearm are not in the same line; the arm forms a dense angle with the forearm, known as the carrying angle. During flexion, however, the forearm and the hand contribute to accessing the middle line of the body and thus enable the hand to be easily carried to the face.
- The authentic adaptation of the trochlea of the humerus, with its prominences and depressions, to the trochlear notch of the ulna, prevents any lateral movement.
- Flexion in the humeroulnar joint is formed by the action of the biceps brachii and brachialis, encouraged by the brachioradialis, with a little contribution from the muscles arising from the medial epicondyle of the humerus.
- Extension in the humeroulnar joint is composed of the triceps brachii and anconeus muscle, with a tiny contribution from the muscles originating from the lateral epicondyle of the humerus, such as the extensor digitorum muscle.
- normal range of flexion and extension is o degree to 140 degrees but only 30 degrees to 130 degrees is required for activities of daily living
Humeroradial joint
- The humeroradial joint is the joint between the head of the radius and the capitulum of the humerus and is a limited ball-and-socket variety, a hinge type of synovial joint
- The annular ligament predicament the head of the radius to the radial notch of the ulna inhibits any separation of the two bones laterally. Therefore, the humeroradial joint is not functionally a ball and socket joint, even if the joint surface in itself allows movement in all directions.
- The annular ligament defends the head of the radius from dislocation, which would otherwise tend to happen, from the shallowness of the cup-like surface on the head of the radius. Without an annular ligament, the tendon of the biceps brachii would be obligated to snatch the head of the radius out of the joint.
- The head of the radius is not in complete contact with the capitulum of the humerus in all positions of the humero radial joint.
- The capitulum amuses only the anterior and inferior surfaces of the lower end of the humerus so that in complete extension a part of the radial head can be simply noticed protruding at the back of the joint.
- In full flexion, the movement of the radial head is captured by the compression of the surrounding soft parts, so that the complimentary rotatory movement of the radius on the humerus is pronation and supination take place in semiflexion, in semiflexion the two articular surfaces are in most intimate contact.
- flexion and extension of the elbow joint are restricted by the tension of the structures on the front and back of the joint; the limitation of flexion is also approved by the soft structures of the arm and the forearm coming into contact.
Proximal radioulnar joint
- The proximal radioulnar joint is a synovial joint that attaches to the proximal ends of the radius and ulna.
- In this joint, the circumferent head of the radius is placed within the ring formed by the radial notch of the ulna and the annular ligament. This arrangement makes this joint a pivot joint.
- The proximal radioulnar joint is a uniaxial joint, that permits movements in one degree of freedom; pronation-supination. In the human being, pronation and supination are unique for the upper limb
- normal range of motion of the proximal radioulnar joint is 180 degrees in which supination is 80 to 90 degrees and pronation is 90 degrees but only 100 degrees ROM is considered for the activity of daily living 50-degree supination and 50-degree pronation
- Blood supply The blood supply to the proximal radioulnar joint comes from a periarticular network formed by the radial collateral branch of the deep brachial artery, and radial and recurrent divisions of the radial and common interosseous arteries.
- movement The proximal radioulnar joint works in a unit with the distal radioulnar joint to enable rotatory movements of the forearm; pronation and supination. When the arm is in the resting position adjoining the body, the range of motion for pronation is 61–66° degrees, while for supination it is 70–77° degrees
- The proximal radioulnar joint takes a closed-packed position at 5° of supination. The open-packed (resting) situation occurs when the forearm is flexed at 70° and supinated at 35°. The capsular pattern of the joint is interpreted and restricted by pronation and supination. The proximal radioulnar joint permits the accessory movements of anteroposterior gliding of the radial head against the ulna and the capitulum of the humerus.
- The muscles that act on the proximal radioulnar joint to produce pronation are the pronator quadratus and pronator teres. The force of the pronator quadratus is enough for gentle movements, while the pronator teres is involved in fast movements and movements against resistance.
- Supination is formed by the contraction of the supinator muscle when the forearm is extended. For the movements against resistance and when the forearm is flexed, the biceps brachii muscle acts as an accessory supinator.
- Blood supply of the proximal radioulnar joint is deep brachial, radial, and common interosseous arteries
Distal radioulnar joint
- The distal radioulnar joint is a pivot-type synovial joint extant in the middle of the ulnar notch of the distal radius and the head of the ulna. The primary confluent structure of the joint is the articular disc of the distal radioulnar joint, also labeled the triangular ligament part of the Triangular fibrocartilage complex
- movement of the distal radioulnar joint is pro-supination, rotation of the lower end of the radius around an axis which going through the center of the head of the ulna. When the radius rotates forward, pronation of the forearm and hand is the result; and backward supination.
- blood supply and nerve supply are anterior and posterior interosseous nerve
- The muscles which are pronate the forearm at the distal radioulnar joint are the pronator quadratus and pronator teres. The pronator quadratus can bring out the movement when it’s not resisted, but the pronator teres is necessary for quick movements and movements against resistance.
Conditions required mobilization of the elbow joint
- Cubital Tunnel Syndrome
- Ligamentous Injuries
- Lateral Epicondylitis
- Medial Epicondylitis
- Olecranon Bursitis
- Olecranon Fracture
- Osteochondritis Dissecans of the Elbow
- Radial Head Fracture
- Ulnar Nerve Entrapment
- Rheumatoid Arthritis
Goals for elbow joint mobilization
pain, muscle guarding, and spasm
- painful joint, reflex, muscle guarding, and muscle spasm can be mediated with gentle joint play techniques to stimulate neurophysiological and mechanical effect
Neurophysiological effect
- small amplitude oscillatory and distraction movement are acclimated to stimulate mechano receptors that may inhibit the transmission of nociceptive stimuli at the spinal cord or brain stem level
Mechanical effect
- small amplitude distraction or gliding movement of the joint is acclimated cause synovial fluid motion, which is a vehicle for carrying nutrients to avascular portions of the articular cartilage
- gentle joint play procedures help to maintain nutrient exchange and prevent the painful and degenerating effects of statis when the joint is swollen or painful, and can not go through a range of motion
- when adapted to treat pain, muscle spasms, and muscle guarding these techniques should not place stretch on the reactive tissue
Reversible joint hypomobility
- reversible joint hypomobility can be mediated with progressively vigorous joint play stretching procedure to elongate hypermobile capsular and ligamentous connective tissue
- sustained or distraction stretch forces are acclimated to distend the shortened tissue mechanically
Positional faults/subluxations
- A faulty position of one bony partner about its opposing surface may outcome in limited motion or pain
- positional faults can occur with traumatic injury, after periods of immobility, muscle imbalance
- the faulty position may be preserved by maladapted neuromuscular control across the joint
- during attempting an active range of motion, faulty tracking of the joint surface results in pain or limited motions
Progressive limitations
- diseases that progressively restrict movement can be treated with joint play techniques to maintain available motion or lessen progressive mechanical restrictions
- the patient’s response manner the dosage of distraction or glide to treatment and the state of the disease
functional immobility
- when the patient can’t functionally move a joint for a longer period
- the joint can be mediated with nonstretch gliding or distraction procedure to maintain available joint play and prevent the degenerating and restricting effect of immobility
Grades of mobilization of the elbow joint
Non-thrust oscillation techniques
- the oscillation may be performed using physiological movement
- grade 1:small amplitude rhythmic oscillation is applied at the beginning of the range, rapid oscillation like manual vibration
- grade 2:large amplitude rhythmic oscillation is done within range, not reach the limit, perform 2 or 3 seconds for 1 to 2 minutes
- grade3:large amplitude rhythmic oscillation is applied up to an available range of motion, stress into tissue resistance, perform 2 or 3 seconds for 1 to 2 minutes
- grade4:small amplitude rhythmic oscillation is executed at the available range of motion, the stress in tissue resistance, rapid oscillation like manual vibration
- grade 1 and 2 are used to treat joint limitation of movement by pain or muscle guarding
- grade 3 and 4 are helpful for stretch maneuver
Nonthrust sustained joint play techniques
- This system interprets only joint play techniques that separate (distract) or glide the joint surface
- grade 1(loosen): small amplitude distraction is applied when no stress is placed on the capsule, it equalizes cohesive force, muscle tension, and atmospheric pressure acting on joint
- grade2(tighten): enough distraction or glide is applied to tighten the tissue surrounding the elbow joint
- grade3(stretch): a distraction or glide is applied with an amplitude large enough to put a stretch on the joint capsule surrounding the periarticular structure
- grade 1 distraction is applied with all glide motion
- apply periodic distraction for 7 to 10 seconds with a few seconds of rest in between several cycles
- grade 2 distraction is helpful to determine the sensitivity of the joint, once the joint reaction is known treatment dosage increases and decreases
- gentle grade 2 distraction apply periodically used to prevent pain and maintain joint play when ROM is not allowed
- grade 3 distractions or glides are helpful to stretch joint structure, increase joint play motion
- For restricted joints apply a minimum of 6 seconds of stretch force chased by partial release (grade 1 or 2)
- reps:3 to 4-second intervals
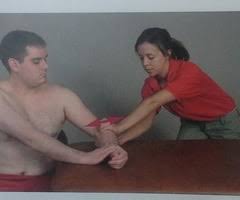
Humeroulnar mobilization
- the convex trochlea articulates with concave olecranon fossa
- resting position: elbow is flexed 70 degrees, forearm supinated 10 degrees
- treatment plane: olecranon fossa angled approximately 45 degrees from the long axis of the ulna
- stabilization: fixate the humerus opposed to the treatment table with a belt or use an assistant to hold it
- the patient may roll onto his/her side and fixate the humerus with the contralateral hand if muscle relaxation can be maintained around the elbow joint being mobilized
Humeroulnar distraction and progression

- patient position: supine with an elbow over the edge of the treatment table or supported with padding just proximal to the olecranon process
- rest the patient’s wrist against your shoulder allowing the elbow to be in resting position for initial treatment
- to stretch into either flexion or extension position of the joint at the end of its available range
Therapist position and hand placement
- when in the resting position or at end range flexion place the fingers of your medial hand over the proximal ulna on the volar surface and reinforce it with your other hand
- to isolate the mobilization force to the humeroulnar articulation, be sure that the writing hand isn’t in contact with the proximal radius
- during at end range extension, stand and place the base of your proximal hand over the proximal portion of the ulna and support the distal forearm with your other hand
mobilizing force
- Apply force against the proximal ulna at a 45-degree angle to the shaft of the bone
- This glide is used to reduce pain ( grade 1 or 2 ), increase flexion or extension (grade 3 or 4)
Humeroulnar distal glide

patient position and hand placement
- supine with an elbow over the edge of the treatment table
- begin with the elbow in the resting position
- progress by positioning the elbow at the end range of flexion
- place the finger of your medial hand over the proximal ulna on the volar surface and reinforce it with another hand
- to isolate the mobilization force of the humeroulnar articulation
- be sure that the writing hand isn’t in contact with the proximal radius
mobilizing force
- first, apply a distraction force to the joint at a 45-degree angle to the ulna
- while maintaining distraction direct the force in a distal direction along the long axis of the ulna using a scooping motion
- This glide is used to increase flexion
Humeroulnar radial glide

- patient position: side lying on the arm which is mobilized
- shoulder laterally rotated, the humerus supported on the table
- begin with an elbow in resting position and progress to end range flexion
hand placement
- place the base of your proximal hand just distal to the elbow, and support the distal forearm with your other end
mobilizing force
- Apply force opposed to the ulna in a radial direction
- This glide is used for an accessory motion of the joint that accompanies elbow flexion
Humeroulnar ulnar glide

- patient position: side lying on the arm which is mobilized
- block or wedge shape thing is put under the proximal forearm for stabilization, using distal stabilization
- the elbow is placed in a resting position and progresses to end range extension
mobilizing force
- Apply force opposed to the distal humerus in a radial direction, causing the ulna to glide ulnarly
- This glide is used to increase valgus force, and this is an accessory motion of the joint that accompanies elbow extension
Humeroradial mobilization
- The convex capitulum vocalizes with the concave radial head
- Resting position: elbow is extended and forearm is supinated to the end of available range
- Treatment plane: the concave radial head perpendicular to the long axis of the radius
- Stabilization: fixate the humerus with one of your hand
Humeroradial distraction

- patient position: supine or sitting, with the arm relax on the treatment table
therapist position and hand placement
- position of the therapist on the ulnar side of the patient’s forearm
- so the position of the therapist between the patient’s hip and upper extremity
- stabilize the patient’s humerus with the superior hand
- grasp around the distal radius with the finger and thenar eminence of the inferior hand
- be sure not to grasp around the distal ulna
mobilizing force
- drag the radius distally, long axis traction causes joint traction
- humeroradial distraction is used to increase the mobility of joints, to manipulate a pushed elbow (proximal displacement of the radius )
Humeroradial dorsal/volar glide

- patient position: supine or sitting with the elbow extended and supinated to the end of the available range of motion
Therapist position and hand placement
- stabilize the humerus with the hand that is on the medial side of the patient’s arm
- place the palmar surface of the therapist’s lateral hand on the volar aspect
- place the fingers on the dorsal aspect of the radial head
mobilizing force
- move the radial head dorsally with the palm of your hand or volar with your fingers
- if a stronger force is needed for volar glide, realign your body and push with the base of your hand against the dorsal surface in a volar direction
- humero radial dorsal glides are used to increase elbow extension
- humero radial volar glides are used to increase elbow flexion
Humeroradial compression

- patient position: sitting or supine
therapist position and hand placement
- approach the patient’s right hand to the therapist’s right hand and the patient l’s left hand to the therapist’s left hand
- stabilize the elbow posteriorly with another hand
- if the supine position stabilizes the hand under the elbow supported on the treatment table
- place your thenar eminence opposed to the patient’s thenar eminence (locking thumbs )
mobilizing force
- simultaneously, extend the patient’s wrist push opposed to the thenar eminence, and compress the long axis of the radius while supinating the forearm
- humero radial compression is used to reduce pulled elbow subluxation
Proximal radioulnar joint mobilization
- the convex rim of the radial head vocalizes with the concave radial notch on the ulna
- resting position: the elbow is flexed position 70 degrees, and the forearm is supinated position 35 degrees
- treatment plane: the radial notch of the ulna parallel to the long axis of the ulna
- stabilization: the proximal ulna is stabilized
Proximal radioulnar dorsal and volar glide
- patient position: sitting or supine begin with the elbow flexed 70 degrees and the forearm supinated 35 degrees
- progress by placing the forearm at a limited range of pronation and supination prior to administering the respective glide
therapist position and hand placement
- approach the patient from the volar and dorsal aspect of the forearm
- fixate the ulna with your medial hand and surround the medial aspect of the forearm
- with your other hand grasp the head of the radius between your flexed fingers and the palm of your hand
mobilizing force
- force the radial head volarlly and dorsally by pushing with your palm or pulling with your finger
- if a stronger force is needed rather than pulling with your fingers move to another side of the patient
- move your hands and apply the force with the palm of your hand
- proximal radioulnar volar glide is used to increase pronation
- proximal radioulnar dorsal glide is used to increase supination
Distal radioulnar joint mobilization
- the concave ulnar notch of the radius vocalizes with the convex head of the ulna
- resting position: forearm is supinated 10 degree
- treatment plane: the treatment plane is articulating surface of the radius, parallel to the long axis of the radius
- stabilization :distal ulna
Distal radioulnar dorsal and volar glides

- patient position: sitting with the forearm placed on the treatment table
- begin with resting position and progress to the end range of pronation or supination
therapist position and hand placement
- stabilize the distal ulna by placing the fingers of one hand on the dorsal surface of the thenar eminence
- the thumb on the volar surface
- place the other hand in the same manner around the distal radius
mobilizing force
- glide the distal radius dorsally to increase supination, volar to increase pronation parallel to the ulna
Precaution for mobilization of the elbow joint
Hypermobility
- the joint of a patient with potential necrosis of the ligaments should not be mobilized with stretching techniques
Joint effusion
- the joint effusion by reason of trauma or disease
- rapid swelling of the joint usually indicates bleeding in the joint and may occur with diseases like hemophilia
- medical intervention is required for aspiration of the blood to reduce the necrotizing effect on the articular cartilage
- slow swelling for more than 4 hours usually specifies serious joint effusion or edema on the joint due to mild trauma irritation or disease such as arthritis
- do not stretch swollen joint with mobilization because the capsule is already stretched by being distended to contain the extra fluid
- the restriction of motion is from extra fluid and muscle response to pain, not from shortened fibers
- gentle oscillating motion that does not stress or stretch the capsule may help to block the transmission of a pain stimulus so it is not perceived and may help to recover fluid flow during maintaining available joint play
- if the patient’s response to gentle techniques is increased pain or joint irritability
- the techniques were applied too vigorously or should not do with the current state of pathology
Inflammation
- whenever inflammation is present, stretching cause increase pain and muscle guarding and result in greater tissue damage
- gentle distraction motions may temporarily prevent the pain response
FAQS
- can elbow stiffness go away with the mobilization?
Elbow mobilization is verified to be effective in post-traumatic or post-operative elbow injury cases.
- can mobilization of the elbow be good before surgery ??
Early mobilization decreases the risk of postoperative complications, accelerates the recovery of functional capacity, positively impacts several patient-reported outcomes, and decreases hospital length of stay, thereby reducing care costs.
- Why is early mobilization important after an injury?
In patients with acute limb injuries, early mobilization decreases pain and swelling and improves functional outcomes correlated with cast immobilization
- How does joint mobilization reduce pain?
grade 2:large amplitude rhythmic oscillation is done within range, not reaching the limit, perform 2 or 3 seconds for 1 to 2 minutes
that transfer midway into the joint range of motion, occupying any part of the range and yet not reaching the end range. This technique can be applied to treat joint stiffness by increasing the range of motion and joint pain - How long do you do joint mobilization for the elbow?
Typical treatment of an elbow joint may include a series of three to six mobilizations persisting up to 30 seconds, with one to three oscillations or glide per second