
Axillary Nerve
Table of Contents
What is Axillary Nerve?
The axillary nerve is one of the terminal branches brachial plexus, derived from its posterior cord (C5-6). It travels through the quadrangular space along with the posterior arterial blood vessel and vein.
It is a mixed nerve, meaning that it’s both motor and sensory fibers that innervate important muscles of the upper limb and parts of the skin within the axillary region.
It also innervates the glenohumeral joint, and because of their close spatial relation, the nerve is commonly injured whenever the joint is injured. The injuries of the axillary nerve result in decreasing or complete loss of function within the structures that it innervates.
This article will discuss the anatomy and performance of the axillary nerve, followed by any clinical pathology associated with this nerve.
Origin
The axillary nerve arises as a terminal branch of the posterior cord of the brachial plexus. The brachial plexus is created by the anterior/ventral rami (roots) of spinal nerves C5-C8 (a.k.a. 5th-8th cervical nerves), together with the anterior ramus of the primary spinal nerve (T1). These five roots combine to make three trunks, the superior (C5-6), middle (C7), and inferior (C8-T1).
These three trunks then divide into anterior and posterior divisions which then reform to lead to three cords. There are five terminal branches of the plexus brachialis derived from these cords. one of all these terminal branches is the axillary nerve.
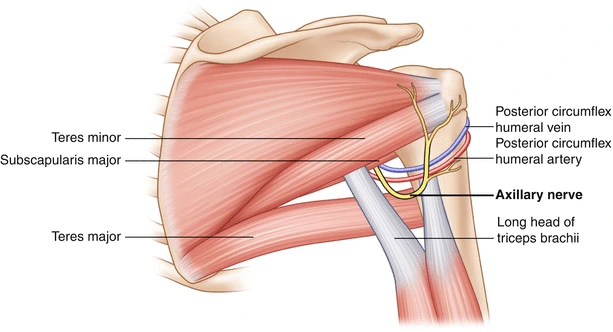
The axillary nerve branches from the posterior cord (C5 – T1) and descends within the axilla posterior to the arterial blood vessel and anterior to the subscapularis. It emerges from the axilla at the extent of the lower border of the subscapularis, by traversing the quadrangular space. this can be an area within the posterior scapular region, which is bounded by the superior margin of the teres inferiorly, the inferior margin of the musculus teres minor superiorly, the lateral margin of the long head of the triceps medially, and therefore the surgical neck of the humerus laterally. Here, it supplies a branch to the articulatio humeri. The posterior circumflex humeral artery and vein also run rearward to the current nerve during this space.
Anatomical Course
The axillary nerve is made within the axilla area of the upper limb. it’s an instantaneous continuation of the posterior cord from the plexus brachialis – and thus contains fibers from the C5 and C6 nerve roots.
In the axilla, the axillary nerve is found posterior to the arteria and anterior to the subscapularis muscle. It exits the axilla at the inferior border of subscapularis via the quadrangular space, often in the course of the posterior circumflex humeral artery and vein.
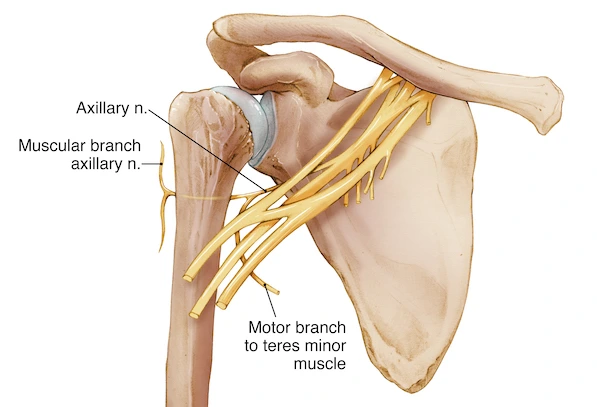
The axillary nerve then moves medially to the surgical neck of the humerus, and it is divided into three terminal branches:
Posterior terminal branch – provides motor innervation to the posterior aspect of the striated muscle and teres. It also innervates the heal the inferior part of the deltoid because of the upper lateral cutaneous nerve of the arm.
Anterior terminal branch – turns round the surgical neck of the humerus and gives motor innervation to the anterior aspect of the deltoid and then it terminates with cutaneous branches to the anterior and anterolateral shoulder.
Articular branch – supplies the glenohumeral joint
Structure
The nerve lies initially behind the arterial blood vessel, and ahead of the subscapularis, and passes downward to the lower border of that muscle.
It then winds from anterior to posterior round the neck of the humerus, in company with the posterior humeral arterial blood vessel, through the quadrangular space (bounded above by the teres, below by the teres muscle, medially by the long head of the musculus triceps brachii, and laterally by the surgical neck of the humerus), and divides into an anterior, a posterior, and a collateral branch to the long head of the musculus triceps brachii branch.
The anterior branch (upper branch) winds round the surgical neck of the humerus, beneath the deltoid, with the posterior humeral circumflex vessels. It continues as far because the anterior border of the deltoid supplies motor innervation. The anterior branch also gives off some small cutaneous branches, which pierce the muscle and provide within the overlaying skin.
The posterior branch (lower branch) supplies the musculus teres minor and therefore the posterior part of the deltoid. The posterior branch pierces the deep fascia and continues because the superior (or upper) lateral cutaneous nerve of the arm, which sweeps round the posterior border of the deltoid and supplies the heal the lower two-thirds of the posterior part of this muscle, yet as that covering the long head of the triceps.
The motor branch of the long head of the musculus triceps brachii arises, on average, a distance of 6 mm (range 2–12 mm) from the terminal division of the posterior cord termination.
The trunk of the axillary nerve gives off an articular filament which enters the articulatio spheroidea below the subscapularis.
Variation
Traditionally, the axillary nerve is believed to only supply the deltoid and teres. However, several studies on cadavers distinguished that the long head of musculus triceps brachii is innervated by a branch of the axillary nerve.
Functions
Motor Functions
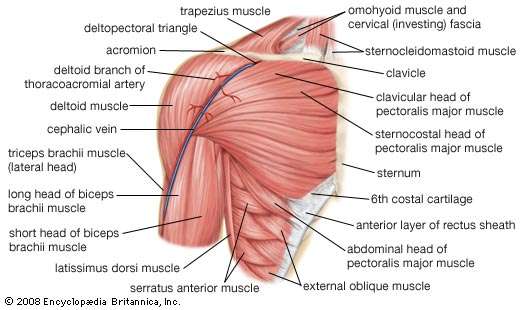
The axillary nerve innervates teres and deltoid muscles.
Teres minor – Teres minor is a part of the structure muscles which act to stabilize the glenohumeral joint. It acts to externally rotate the cotyloid joint and is innervated by the posterior terminal branch of the axillary nerve.
Deltoid muscle– deltoid is situated at the superior aspect of the shoulder. It accomplishes abduction of the upper limb at the glenohumeral joint and is innervated by the anterior terminal branch of the axillary nerve.
Sensory Functions
The sensory factor of the axillary nerve is delivered through its posterior terminal branch.
After the posterior terminal branch of the axillary nerve has innervated the teres minor muscle, it continues because of the upper lateral cutaneous nerve of the arm. It innervates the heal the inferior portion of the deltoid (the ‘regimental badge area’).
With axillary nerve damage, a sensation at the regimental symbol area could also be damaged or absent. The patient can also report paraesthesia (pins and needles) within the distribution of the axillary nerve.
Clinical significance
The axillary nerve is also injured in anterior-inferior dislocations of the ball-and-socket joint, compression of the axilla with a crutch, or fracture of the surgical neck of the humerus. For instance, injury to the axillary nerve includes axillary nerve palsy.
Isolated damage to the axillary nerve ends up in mononeuropathy, a sort of peripheral neuropathy where just one nerve is engaged. Potential causes include direct trauma to the nerve, pressure on the nerve from infringement of around anatomical structures, or shoulder injury.
For athletes who participate in real sports, damage to the axillary nerve is that the commonest peripheral nerve injury. An injury to the axillary nerve may be thanks to dislocation of the articulatio humeri because the two are in close proximity to each other. Lesions to the nerve can even occur in a very fracture of the surgical neck of the humerus. During shoulder operations, the axillary nerve is prone to damage and this will be a complication of those surgeries.
Injury to the axillary nerve may end up within the following:
- Paralysis of the deltoid and teres muscle muscles
- Weakness of arm abduction
- Wasting of the deltoid
- Anesthesia or loss in the sensation of the world of the skin posterior to the deltoid
- Atrophy of the skeletal muscle leads to a loss of the conventional rounded appearance of the shoulder, which provides the shoulder a flattened appearance.
Damage to the 5th and 6th spinal cervical nerves during delivery of a neonate leads to Erb’s palsy. Since the axillary nerve stems from the upper trunk of the nerve plexus (C5-C6), the infant cannot abduct nor externally rotate the arm at the shoulder joint.
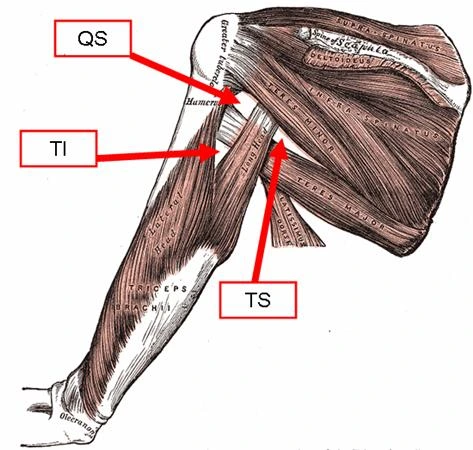
The Quadrangular Space
The quadrangular space may be a gap within the muscles of the posterior scapular region. it’s a pathway for neurovascular structures to maneuver from the axilla anteriorly to the posterior shoulder and arm. Quadrangular Space Syndrome can cause weakness of the skeletal muscle but more commonly leads to atrophy of the teres muscle. This syndrome occurs when the muscles of the quadrangular space hypertrophy and thus hit the axillary nerve during this space.
It is bounded by:
- The superior-inferior aspect of teres minor
- The inferior – superior aspect of teres major
- The lateral – surgical neck of the humerus.
- The medial–long head of musculus triceps brachii
- Anterior – subscapularis
The axillary nerve and posterior circumflex humeral artery and vein taste the quadrangular space. These structures will be compressed as a result of trauma, muscle hypertrophy, or space-occupying lesion; leading to weakness of the deltoid and teres minor muscle. this can be particularly common in athletes who perform overhead activities.
Injury to the Axillary Nerve
The axillary nerve may be damaged through trauma to the proximal humerus or arch. It often presents with other nerve plexus injuries.
Common appliances of injury include fracture of the humeral surgical neck, shoulder dislocation, or iatrogenic injury while shouldering surgery.
Motor functions – the deltoid and teres muscles will be affected, rendering the patient unable to abduct the affected limb beyond 15 degrees.
Sensory functions – the upper lateral cutaneous nerve of the arm is affected, leading to loss of sensation over the inferior deltoid.
Clinical tests involve deltoid extension lag and external rotation lag. Chronic lesions of the axillary nerve may end up in permanent numbness in the lateral shoulder region, muscle atrophy, and neuropathic pain.
Erb’s Palsy
Erb’s palsy could be a condition resulting from damage to the C5 and C6 roots of the plexus brachialis. The axillary nerve is affected, and the person is irregularly incapable of abducting or externally rotating at the shoulder.
It commonly occurs when there’s an excessive increase in the angle between the neck and shoulder, which stretches the nerve roots. The severity of the injury stretches from neuropraxia to avulsion, which decides recovery.
FAQ
Where are axillary nerves located?
The axillary nerve starts in the neck and then extends to the shoulder. It leads to movement and sensation in the shoulder and the back of your upper arm. Injuries to the present nerve can affect the ability to rotate the arm or lift it.
What muscles are controlled by the axillary nerve?
The axillary nerve has both a motor and a sensory allocation of innervation. it’s motor fibers that innervate the striated muscle, acting as an abductor, flexor, and extensor at the shoulder, furthermore because the teres minor muscle, allowing lateral rotation of the glenohumeral joint.
What happens when an axillary nerve is damaged?
Axillary nerve dysfunction is nerve damage that may cause a loss of movement or sensation within the shoulder. Conditions connected to axillary nerve dysfunction involve a fracture of the humeruspressure from casts or splints and improper use of crutches.
Can axillary nerve damage be repaired?
In many cases, Nerve injury will heal on its own. this could take several months. During that point, it’s important to try to do therapy to take care of flexibility across the spheroid joint. If after several months, the weakness doesn’t improve, then surgery to treat the nerve injury is indicated.
Is axillary nerve damage serious?
In traumatic shoulder injury involving the axillary nerve, most patients may recover with non-operative treatment; however, there’s the chance of permanent paralysis. In many cases, when the shoulder is reduced, the requirement for surgical intervention is minimal.

One Comment