Athetoid cerebral palsy | Dyskinetic cerebral palsy
Table of Contents
What is Athetoid/Dyskinetic cerebral palsy?
- Athetoid cerebral palsy also called dyskinetic cerebral palsy, this is the second most common type.
- Intelligence is usually normal, yet muscle problems affect the whole body.
- Fragile or tight muscle tone causes random and uncontrolled body movements.
- The child will have difficulties walking, sitting, maintaining posture, and speaking clearly because the tongue and vocal cords are hard to control.
- Certain children drool if they have problems controlling facial muscles.
- Athetoid cerebral palsy or dyskinetic cerebral palsy (sometimes abbreviated ADCP) is primarily associated with damage to the basal ganglia and the substantia nigra in the form of lesions that happen during brain development and cause bilirubin encephalopathy and hypoxic-ischemic brain injury.
- ADCP is characterized by both hypertonia and hypotonia, caused by the affected individual’s inability to control muscle tone.
- Clinical diagnosis of ADCP typically occurs within eighteen months of birth and is primarily based upon motor function and neuroimaging techniques.
- Athetoid dyskinetic cerebral palsy is a non-spastic and extrapyramidal form of cerebral palsy.
- Dyskinetic cerebral palsy can be divided into 2 different groups; choreoathetosis and dystonic.
- Choreo-athetotic Cerebral palsy is characterized by involuntary movements most predominantly found in the face and extremities.
- Dystonic ADCP is characterized by slow, strong contractions, which may happen locally or encompass the whole body.
What are the types of athetoid cerebral palsy?
- Athetoid cerebral palsy may be given other distinctions to further classify the condition founded on the specific type of involuntary movement.
The various types of athetoid cerebral palsy include:
- Dystonia – Slow and steady, rotational movement of the torso, arm, or leg.
- Chorea – Sudden involuntary movements, mainly in fingers and toes.
- Athetosis – Sluggish, writhing movements, especially in fingers and face.
- Choreoathetoid – A union of the chorea and athetosis.
- Ataxia – Mislying balance and coordination.
- Rigidity – Increase muscle tone due to hypertonia causes restricted movement.
- Dyskinesia is – Common term to describe involuntary movements.
- Athetoid cerebral palsy is frequently interchangeably referred to as dyskinetic cerebral palsy for this reason.
What are the causes of athetoid cerebral palsy?
- The most common cause of athetosis is an injury to the basal ganglia, which is the part of the brain liable for motor control.
- It also influences controlling functions, emotions, behaviors, and motor learning.
- In children, the injury generally happens during or sometime after birth and is a cause of many forms of cerebral palsy.
- Athetosis may occur in adults who have a stroke or severe peripheral neuropathy.
Basal ganglia diseases
- Disease or damage in the basal ganglia part of your brain can generate symptoms of athetosis.
- Your brain loses its capability to smooth out muscle movements or coordinate changes in posture.
- When nerve impulses lack proper control, they lead to uncoordinated muscle movements, abnormal posture, and abnormal improvement in tone.
- Certain diseases that affect this part of the brain include Huntington’s disease and Wilson’s disease.
- Huntington’s is hereditary and makes the brain’s nerve cells malfunction over time.
- Wilson’s disease is an infrequent genetic disorder that leads to copper poisoning in the body.
Birth problems
- If a baby does not get enough air supply during birth, they are at a higher risk of developing athetosis.
- Lack of oxygen results in brain damage and increases dopamine levels in the brain, affecting the basal ganglia.
Jaundice
- If your baby is born with increased levels of bilirubin, they can get basal ganglia damage.
- Treatment assists to lower the amount of the compound.
- However, the blood-brain barrier that protects the body from toxins does not develop properly.
- The bilirubin may even now find its way to the brain and cause damage.
Drug toxicity
- Drugs that increase dopamine levels in the brain can result in damage to the basal ganglia.
- This will show the symptoms of athetosis.
- Cerebral palsy, or CP, happens due to abnormal development of or damage to the brain.
- The result is that a child is not able to control muscle movements.
- Cerebral palsy that occurs due to damage to the basal ganglia is known as athetoid cerebral palsy.
- It can also be for the reason of high bilirubin levels and asphyxia or oxygen deficiency from abnormal breathing.
Stroke
- Involuntary movements may also become apparent from stroke, especially in adults.
- Damage to the brain results from a problem with neuron movement.
- The results are symptoms of athetosis and other disorders related to movements.
What are the symptoms of athetoid cerebral palsy?
- The signs and symptoms of athetosis depend on the level of the damage and the location of movement issues.
- The symptoms develop from problems with high and low muscle tone, which can variable constantly.
- High muscle tone can occur in jerky movements and stiffness.
- On the other hand, low muscle tone leads to muscle floppiness and creates trouble in postures like sitting up.
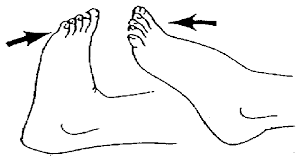
The most frequent symptoms that come with athetosis are:
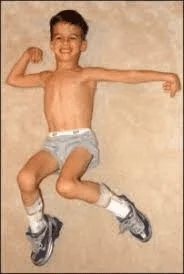
- Slow, writhing, & involuntary muscle movements
- Tremors
- Poor sitting /standing posture
- Unsteadiness
- Quick movements and changes in muscle movements,
- Twisting of the torso
- Grimacing
- Symptoms that get inadequate with attempts at improved posture or controlled movement.
- The symptoms of athetoid Cerebral palsy depend on whether the damage was sole to the basal ganglia, or if both the cerebellum and basal ganglia were damaged.
- If both areas are damaged, this will probably cause problems with balance and coordination.
- Parents and caregivers usually begin noticing signs of involuntary or jerky movements when their child is around nine months or older.
- In many young children, irregular movement may be indicative of a developmental delay, yet not necessarily a sign of cerebral palsy.
Athetoid cerebral palsy may be present in a child who:
- Does not kick legs,
- Looks stiff or rigid,
- Looks limp,
- Does not hold up head at three months old,
- Does not reach for objects,
- Does not smile by three months old,
- Does not roll over.
- There are 3 defining characteristics of dyskinetic cerebral palsy: dystonia, athetosis, and chorea.
- Each of these characteristics happens with its own symptoms.
Dystonia
- Dystonia requires involuntary muscle contractions marked by writhing, slow and repetitive movements that become inadequate when the child begins to move.
Other symptoms include:
- Abnormal and tricky posture,
- Movements that another from slow and painful to fast and rapid,
- Involuntary movements enlarge when the child is stressed or tired.
- Dystonia can affect all parts of the body, but in certain cases, it happens in only one area of the body.
- For example, while one child may have involuntary, awkward movements in the whole body (generalized dystonia), another child may have these same symptoms only in the legs (focal dystonia).
- Many people with dystonia use sensory polys to suppress involuntary movements.
- For example, resting against the wall or placing their hand behind the head can assist certain people with dystonia to control their movements.
- Other sensory ploys involve pressing fingers against the eyes or nose, using a tight headband on the forehead, and placing the hand under the chin.
Athetosis
- Athetosis is another feature of dyskinetic cerebral palsy, marked by slow and steady twitching and wriggling movements.
- The symptoms can surface while resting and commonly become worse when the child moves.
Other common symptoms of athetosis include:
- Involuntary slow, continuous writhing movements which aggravate with attempts to move,
- Fluctuating muscle tone (from stiff to floppy),
- Grimacing & drooling from lack of facial muscle control,
- Difficulties with eating and drinking,
- Problems grasping and holding tiny objects because of changes in muscle tone,
- Involuntary movements may be constant unless the child is totally relaxed,
- Involuntary movements usually disappear when the child is asleep.
Chorea
- Chorea is a characteristic of dyskinetic cerebral palsy marked by short irregular and involuntary movements.
- The name comes from the Greek word, chorea, meaning “dance,” therefore the involuntary movements are often repetitive.
- This can affect different parts of the body.
- Chorea can occur in difficulties with chewing, drinking, swallowing, and speech.
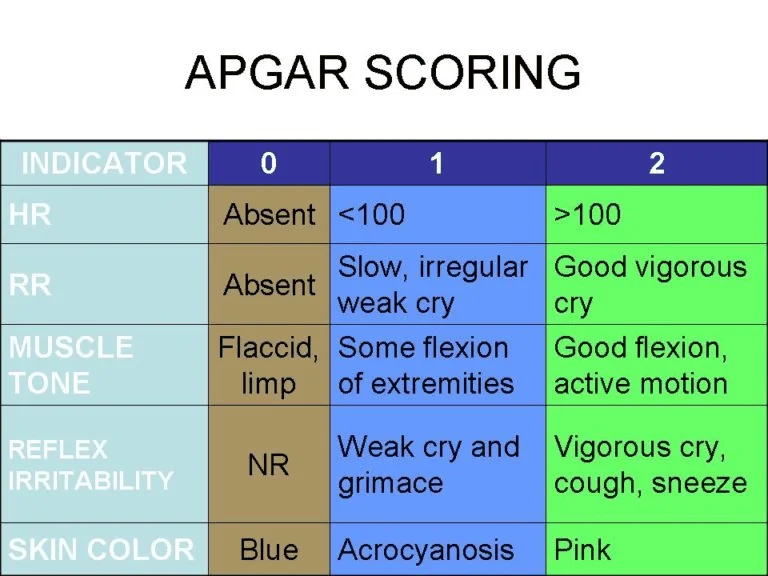
Diagnostic study:
- Physical Assessment.
- Observe LBW, preterm, and those with low Apgar scores at five minutes.
- Observe babies who have seizures, intracranial hemorrhage, and metabolic disturbances.
- Later control of movement does not occur until late infancy, diagnosis may not be confirmed until after six months of age.
Warning signs:
- Physical Signs:
- poor head control after three months,
- stiff or rigid arms or legs, arching back, floppy or limp posture,
- Can’t sit up without support for eight months,
- Uses only one side of the body/only the arms to crawl.
- Behavioral Signs:
- Utmost irritability or crying,
- Failure to smile by three months,
- Feeding difficulties,
- Persistent gagging/choking when fed,
- After six months of age, the tongue pushes soft food outside the mouth.
How is athetoid cerebral palsy diagnosed?
- The symptoms of athetoid Cerebral palsy depend on whether the damage was sole to the basal ganglia, or if both the cerebellum and basal ganglia were damaged.
- If both areas are damaged, this will probably cause problems with balance and coordination.
- Parents and caregivers usually begin noticing signs of involuntary or jerky movements when their child is around nine months or older.
- In many young children, irregular movement may be indicative of a developmental delay, yet not necessarily a sign of cerebral palsy.
Athetoid cerebral palsy is possibly present in a child who:
- Does not kick legs,
- Looks stiff or rigid,
- Looks limp,
- Does not hold up head at three months old,
- Does not reach for objects,
- Does not smile by three months old,
- Does not roll over.
- Most children with athetoid cerebral palsy are diagnosed in the first two years of life.
- Health care providers look for signs of Cerebral palsy if a baby is born early or has another health problem that is associated with Cerebral palsy.
- No single test can diagnose athetoid cerebral palsy.
- So health care professionals see at many things, including a child’s:
- development,
- growth,
- reflexes,
- movement.
Testing may include:
- brain MRI, CT scan, or ultrasound,
- blood and urine tests to check for other medical conditions, including genetic conditions,
- electroencephalography (EEG) to seems at electrical activity in the brain,
- electromyography (EMG) to check for muscle weakness,
- evaluation of how a child walks & moves,
- speech, hearing, and vision testing.
- Our age-specific overviews can give you a sense of how your child might develop from birth to age five.
Development
Your Child’s Development: Newborn
- From the moment babies are born, they respond to the world around them.
- Their reactions — being calmed by a parent’s hug or startled by a loud sound — are examples of normal infant development.
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here is what your newborn might do:
- Communication and Language Skills
- turns his or her head side of the parent’s voice or other sounds
- cries to communicate a need (to be held/fed, to have a diaper changed, or need to sleep)
- stops crying when a need is met (when picked up, fed, changed, and put down for a nap)
2. Movement and Physical Development
- moves in response to sights & sounds
- rooting reflex: turns the side of the breast or bottle and sucks when a nipple is placed in the mouth
- Moro reflex (startle response): when startled, stretches arms & legs out, then curls them back in
- fencer’s pose (tonic neck reflex): when the head is turned to one side, straightening the arm on that side while bending the opposite arm
- grasp reflex: holds a finger placed in the palm and toes curl when touched on the sole of the foot
3. Social and Emotional Development
- soothed by a parent’s voice & touch
- has periods of the alertness
4. Cognitive Skills (Thinking & Learning)
- looks at faces when quiet & alert
- follows the faces
When Should I Call the Doctor?
- Every child develops at their admit pace.
- But if something concerns you, tell your doctor.
Additionally, tell the doctor if your baby:
- does not suck well at the breast or on a bottle nipple
- has an arm or leg that looks weaker than the other
- is very fussy/hard to soothe.
Your Child’s Development: 3-5 Days
- Though only a few days old, your baby already is able to interact in certain ways.
- When alert, your baby will probably focus on your face.
- Babies are especially drawn to the higher-pitched voices, so give in to that urge to use “baby talk.”
- You are introducing your baby to language & your baby will enjoy it.
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here is what your newborn might do:
- Communication and Language Skills
- turns his or her head side of the parent’s voice or other sounds
- cries to communicate a need (to be held/fed, to have a diaper changed, or need to sleep)
- stops crying when a need is met (when picked up, fed, changed, and put down for a nap)
2. Movement and Physical Development
- moves in response to sights & sounds
- rooting reflex: turns the side of the breast or bottle and sucks when a nipple is placed in the mouth
- Moro reflex (startle response): when startled, stretches arms & legs out, then curls them back in
- fencer’s pose (tonic neck reflex): when the head is turned to one side, straightening the arm on that side while bending the opposite arm
- grasp reflex: holds a finger placed in the palm and toes curl when touched on the sole of the foot
3. Social and Emotional Development
- soothed by a parent’s voice & touch
- has periods of the alertness
4. Cognitive Skills (Thinking & Learning)
- looks at faces when quiet & alert
- follows the faces
When Should I Call the Doctor?
- Every child develops at their admit pace.
- But if something concerns you, tell your doctor.
Additionally, tell the doctor if your baby:
- does not suck well at the breast or on a bottle nipple
- has an arm or leg that looks weaker than the other
- is very fussy/hard to soothe.
Your Child’s Development: 1 Month
- Have you noticed how your baby’s tiny fingers curl around yours/close into fists?
- how does your small one startle at a loud noise?
- Your baby was born with these and other reflexes, which will get less noticeable as your baby grows.
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here are certain new skills your baby may have:
- Communication and Language Skills
- startles at loud noises,
- makes sounds other than crying.
2. Movement and Physical Development
- keeps hands in tight fists,
- arms and legs move similarly on both sides,
- when lying on the tummy, holds head up shortly.
3. Social and Emotional Development
- recognizes parent’s voice,
- when upset, responds to a parent’s cuddles, voice & affections,
- becomes alert when hearing an affable sound, like music.
4. Cognitive Skills (Thinking and Learning)
- will stare at an object placed in front of the face, specifically something brightly colored,
- follows faces.
When should I call the doctor?
- As your baby becomes more alert, they will watch you constantly.
- And you will be watching your little one closely too.
- So this is an excellent time to watch for any subtle signs that could point to a problem.
Tell the doctor if your baby:
- has one eye that is crossed or eyes that do not line up in the same direction,
- does not respond to pleasing sounds, like as a soft voice or gentle music,
- has legs/hands that do not move in unison: for example, only one leg kicks or just one arm shakes.
Your child’s development: 2 months
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here are things babies commonly do by this age:
- Communication and Language Skills
- produce sounds other than the crying,
- react to the noisy noises.
2. Movement and Physical Development
- when on their belly, clasp up their head,
- move both arms & both legs,
- open their hands shortly.
3. Social and Emotional Development
- calm down when spoken to and picked up,
- look like your face,
- look happy to see you,
- smile when you talk or smile.
4. Cognitive Skills (Thinking and Learning)
- watch you as you move,
- seems at a toy for several seconds.
When should I call the doctor?
- You know your baby best.
- Share your cares — even little ones — with your baby’s doctor.
- If your baby is not meeting one or more milestones or you notice that your baby has skills yet has lost them, tell the doctor.
Your child’s development: 4 months
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here are things babies commonly do by this age:
- Communication and Language Skills
- create sounds like ooh and aah (cooing),
- turn their head toward your voice,
- create sounds in response to being spoken to.
2. Movement and Physical Development
- use their arms to swing at the toys,
- bring their hands to the mouth,
- grasp a toy when you put it in their hand,
- grasp their head steady without support when being held,
- push up on elbows or forearms when on their stomach.
3. Social and Emotional Development
- smile to get your attention,
- chuckle (not a full laugh) when you attempt to make them laugh,
- look at you, move or make the sounds to get or keep your attention.
4. Cognitive Skills (Thinking and Learning)
- look at their hands with interest,
- when hungry, open their mouth if a breast or bottle approaches.
When should I call the doctor?
- You know your baby best.
- Share your cares — even little ones — with your baby’s doctor.
- If your baby is not meeting one or more milestones or you notice that your baby has skills yet has lost them, tell the doctor.
Your child’s development: 6 months
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here are things babies commonly do by this age:
- Communication and Language Skills
- acquire turns making sounds with you,
- blow the raspberries,
- create squealing noises.
2. Movement and Physical Development
- roll from stomach to back,
- push up with straight arms when on their stomach,
- lean on their hand to sit with the support.
3. Social and Emotional Development
- know familiar people,
- enjoy watching in a mirror,
- chuckle.
4. Cognitive Skills (Thinking and Learning)
- put things in their mouth to explore,
- reach to the grab a toy,
- close their lips to show they do not want more food.
When should I call the doctor?
- You know your baby best.
- Share your cares — even little ones — with your baby’s doctor.
- If your baby is not meeting one or more milestones or you notice that your baby has skills yet has lost them, tell the doctor.
Your child’s development: 9 months
- Doctors use milestones to talk if a baby is developing as expected.
- There is a broad range of what is considered normal, so some babies may gain skills earlier or later than others.
- Babies who were born prematurely may extend milestones later.
- Always talk with your doctor about your baby’s progress.
Here are things babies commonly do by this age:
- Communication and Language Skills
- create different sounds like “ba-ba-ba” or “ma-ma-ma”,
- raise their arms to be picked up,
- Movement & Physical Development,
- acquire into a sitting position without any help,
- sit without any support,
- use their fingers to “rake” food toward them,
- pass things from one hand to the others.
2. Social and Emotional Development
- are shy, clingy, or fearful of strangers,
- see, reach for or cry when caregivers leave,
- see when you call their name,
- show several facial expressions, like as happy, sad, angry, and surprised,
- smile/laugh when you play peek-a-boo.
3. Cognitive Skills (Thinking and Learning)
- look for objects when dropped out of sight,
- bang two things together, like blocks.
When should I call the doctor?
- You know your baby best.
- Share your cares — even little ones — with your baby’s doctor.
- If your baby is not meeting one or more milestones or you notice that your baby has skills yet has lost them, tell the doctor.
Your Child’s Development: 1 Year (12 Months)
- Doctors use certain milestones to describe if a toddler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Toddlers who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things toddlers commonly do by this age:
- Communication and Language Skills
- call caregiver “mama” or “dada” or another special name,
- waving goodbye,
- understand “no” (pause/stop when you say it).
2. Movement and Physical Development
- pull up to the stand,
- walk holding onto the furniture (cruising),
- with assistance, drink from a cup without a cover,
- pick up things like small pieces of food with their thumb and forefinger.
3. Social and Emotional Development
- play pat-a-cake & other games.
4. Cognitive Skills (Thinking and Learning)
- put something into a container, like a block in a cup,
- look for things that they see someone hide, like a toy under a blanket.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your toddler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 15 Months
- Doctors use certain milestones to describe if a toddler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Toddlers who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things toddlers commonly do by this age:
- Communication and Language Skills
- point to inquire about something or to get help,
- try to say one or two words (besides “mama” and “dada”), like a “ba” for the ball,
- look at the familiar object when you name it,
- follow directions when given with both a gesture & words.
2. Movement and Physical Development
- take some steps on their own,
- use their fingers to feed themselves.
3. Social and Emotional Development
- show affection to the caregivers with hugs and kisses,
- show caregivers object that they like,
- hug stuffed dolls or teddy bears or other toys,
- similar things doing other children while playing,
- applaud when excited.
4. Cognitive Skills (Thinking and Learning)
- stack at least two small things, like blocks,
- try to use things the right way, like a phone or book.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your toddler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 1.5 Years (18 Months)
- Doctors use certain milestones to describe if a toddler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Toddlers who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things toddlers commonly do by this age:
- Communication and Language Skills
- try to say three or more words (besides “mama” and “dada”),
- follow one step to the directions said with words & not gestures (“Pick up the toy.”).
2. Movement and Physical Development
- walk without holding on to anyone or anything,
- climb on & off a chair or couch without help,
- drink from a cup without a cover and may spill sometimes,
- use their fingers and maybe a spoon for the eat,
- scribble.
3. Social and Emotional Development
- point to show you something interesting,
- move away from you, yet look to make sure you are close by,
- puts hands out to get them washed,
- help with getting dressed by pushing their arm through a sleeve or lifting up to a foot,
- look at some pages in a book with caregivers.
4. Cognitive Skills (Thinking and Learning)
- copy you doing chores, like as sweeping,
- play with toys in a simple way, like pushing a toy car,
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your toddler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 2 Years (24 Months)
- Doctors use certain milestones to describe if a toddler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Toddlers who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things toddlers commonly do by this age:
- Communication and Language Skills
- say at least 2 words together, like “more milk”,
- point to the things in a picture book when asked (“Where is the dog?”),
- point to a minimum of two body parts when asked (“Where is your nose?”),
- use more gestures, like blowing a kiss or nodding yes.
2. Movement and Physical Development
- run,
- kicking the ball,
- walk (not climb) up some stairs with or without help,
- eat with a spoon.
3. Social and Emotional Development
- notice when others are hurt or upset, like as pausing or looking sad,
- See your face to see how to react to a new situation.
4. Cognitive Skills (Thinking and Learning)
- grasp something in one hand while using the other, like as holding a container and taking the lid off,
- try to use switches, knobs, or buttons on the toy,
- play with more than one toy at a time, like putting toy food on a toy plate.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your toddler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 2.5 Years (30 Months)
- Doctors use certain milestones to describe if a toddler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Toddlers who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things toddlers commonly do by this age:
- Communication and Language Skills
- say around fifty words,
- say two or more words together, with one action word, like “doggie run”,
- say words like an “I,” “me,” or “we”,
- address things in a book when you point & ask “What is this?”
2. Movement and Physical Development
- take certain clothes off by themselves,
- jump with both feet,
- use hands to twist things, like turning a doorknob or unscrewing a lid,
- turns pages in a book one at a time.
3. Social and Emotional Development
- play next to other children & sometimes play with them,
- expose you what they can do by saying “Look at me!”,
- follow simple routines when told, like picking up toys when you say “It’s clean-up time.”
4. Cognitive Skills (Thinking and Learning)
- use things to pretend, like feeding a block to a doll as if it were food,
- show simple problem-solving, like using a stool to reach something,
- follow 2-step instructions (“Pick up the toy and put it on the shelf.”),
- know at least one color, like pointing to a red crayon when asked “Which one is red?”
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your toddler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 3 Years (36 Months)
- Doctors use certain milestones to describe if a preschooler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Kids who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things preschoolers commonly do by this age:
- Communication and Language Skills
- say the first name when asked,
- talk with you in conversation with at least two back-and-forth exchanges,
- inquire who, where, or why questions,
- say what action is happening in the picture when asked, like as running, eating, or playing,
- talk well sufficient for others to understand most of the time.
2. Movement and Physical Development
- string items together, like as large beads or macaroni,
- put on certain clothes by themselves,
- use the fork.
3. Social and Emotional Development
- calm down within ten minutes after you leave,
- see other children and join them to play.
4. Cognitive Skills (Thinking and Learning)
- make a circle when you show them how
- avoid touching hot objects, like a stove, when you warn them.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your preschooler is not meeting one or more milestones or you notice that your child has skills yet has lost them, tell your doctor.
Your Child’s Development: 4 Years
- Doctors use certain milestones to describe if a preschooler is developing as expected.
- There is a wide range of what is considered normal so some children may gain skills earlier or later than others.
- Kids who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things preschoolers commonly do by this age:
- Communication and Language Skills
- say sentences with four or more words,
- say certain words from a song, story, or nursery rhyme,
- speak about at least one thing that happened during the day,
- answer the simple questions, like “What is a crayon for?”
2. Movement and Physical Development
- grab a large ball most of the time,
- assist the serving food; pour drinks with help,
- unbutton certain buttons,
- hold pencil or crayon amid fingers & thumb (not in a fist).
3. Social and Emotional Development
- pretend to be something else during play, such as a teacher, superhero, or animal,
- permission to go play with other children if none are around,
- comfort others who are hurt or sad, like hugging a friend who is crying,
- avoid danger, like jumping from a high playground set,
- likes to be a “helper”,
- changes behavior based on environments, like at a library or playground.
4. Cognitive Skills (Thinking and Learning)
- name some colors,
- talk about what comes next in a well-known story,
- sketch a person with three or more body parts.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your preschooler is not meeting one or more milestones or you notice that your child had skills yet has lost them, tell your doctor.
Your Child’s Development: 5 Years
- Doctors use certain milestones to describe if a preschooler is developing as expected.
- There is a wide range of what is considered normal, so some children may gain skills earlier or later than others.
- Kids who were born prematurely may achieve milestones later.
- Always speak with your doctor about your child’s progress.
Here are things preschoolers commonly do by this age:
- Communication and Language Skills
- describe the story they heard or made up with at least two events,
- answers the easy questions about a story after hearing it,
- keep a conversation going with more than three back-and-forth exchanges,
- use or recognize simple rhymes, like as a bat-cat.
2. Movement and Physical Development
- button certain buttons,
- hop on 1 foot.
3. Social and Emotional Development
- obey rules or take turns when playing games,
- sing, dance, or act for you,
- do simple chores, like clearing the table after eating.
4. Cognitive Skills (Thinking and Learning)
- count to ten,
- name certain letters; name numbers between one and five when you point to them,
- use words about time, like yesterday or tomorrow, morning or night,
- pay attention for 5–10 minutes during activities, like arts and crafts (screen time does not count),
- write certain letters in their name.
When should I call the doctor?
- You see your child best.
- Participate in your concerns — even little ones — with your child’s doctor.
- If your preschooler is not meeting one or more milestones or you notice that your child had skills yet has lost them, tell your doctor.
How is athetoid cerebral palsy treated?
- There is no cure for cerebral palsy.
- Yet resources and therapies can help kids grow and develop to their greatest potential.
- The treatment plan may include:
- physical therapy, occupational therapy, speech therapy,
- leg braces, a walker, and/or a wheelchair,
- medicine for muscle pain or stiffness,
- special nutrition to help the child grow,
- surgery to improve movement in the legs, ankles, feet, hips, wrists, and arms.
Physiotherapy treatment of athetoid cerebral palsy
Treatment Approaches for Athetoid Cerebral Palsy
- An extensive range of therapeutic interventions has been used in treating and managing children with cerebral palsy.
- They appear that there is evidence to support the use and effectiveness of neuromuscular electrical stimulation, while conformation in support of the effectiveness of the neurodevelopmental treatment is equivocal at best.
- The effectiveness of the many other intercessions, including include: sensory integration, body-weight support treadmill training, conductive education, constraint-induced movement therapy, and hyperbaric oxygen therapy used in the treatment of cerebral palsy have not been clearly accepted based on well-controlled trials.
- We provide an outline of salient aspects of popular approaches and interventions used in the management of children with Cerebral Palsy.
- Identifies an extensive range of choices and availability of various techniques which may vary both between therapists and from country to country.
- The table below lists many of the most common physiotherapy and physiotherapy-related approaches utilized in the management of Cerebral Palsy during the past few decades.
Neurodevelopmental Treatment (NDT)
- One of the more popular approaches utilized in the management of cerebral palsy, the Neurodevelopmental Treatment Approach also known as the Bobath Approach, was developed in the 1940s by Berta and Karl Bobath, based on their particular observations working with children with cerebral palsy.
- The basis of this approach is that motor abnormalities seen in children with Cerebral Palsy are due to uncommon development in relation to postural control and reflexes reason for the primary dysfunction of the central nervous system.
- This approach aims to facilitate typical motor development and function and to fend off the development of secondary impairments due to muscle contractures, and joint and limb deformities.
- Although the effectiveness of Neurodevelopmental Treatment in Cerebral Palsy has been questioned by specific published reports, there are certain studies suggesting its efficacy.
Constraint-Induced Movement Therapy (CIMT)
- Constraint-induced Movement therapy is used predominantly in the individual with Hemiplegic Cerebral Palsy to better the use of the affected upper limb.
- The stronger or non-impaired upper limb is immobilized for a variable duration in order to Force the Use of the damaged upper limb over time.
- Antilla et al (2008) identified one high and one lower-quality trial which measured both body functions and structures, and activity and participation outcomes through the use of Constraint-induced Movement therapy.
- Use of a cast with Constraint-induced Movement therapy showed positive effects in the amount and quality of functional hand use in the impaired limb and new emerging behavior as compared to the no-therapy group, yet no effects were found on QUEST.
- The use of a sling during Constraint-induced Movement therapy also had positive effects on functional hand use on the impaired upper limb, time to complete tasks, and speed and dexterity, yet no effects on sensibility, handgrip force, or spasticity.
- Thus Antilla et al (2005) found there is moderate evidence for the effectiveness of Constraint-induced Movement therapy on functional hand use in the impaired upper limb.
- According to Patel (2005), the success of this approach has not been established, in particular in relation to the adverse effects of lengthened immobilization of the normally developing upper limb.
Patterning for athetoid cerebral palsy
- The concept of patterning is established on theories developed during the 1950s and 1960s by Fay, Delacato, and Doman.
- Patterning is established on the principle that typical development of the infant and child progresses through a well-established, pre-determined sequence; with failure to typically complete one stage of development causing impediment or impairment in the development of subsequent stages.
- Established on this principle they suggested that in children with Cerebral Palsy typical motor development can be facilitated by passively repeating and putting the child through the sequential steps of typical development, a process called patterning.
- Parents and other caregivers are taught to carry out this patterning process at home yet the approach is hugely labor-intensive and time-consuming as it requires multiple sessions every day.
- Although Patterning has been utilized for many years of its use is now surely controversial and its effectiveness has not been established.
- It is a very passive therapy, with a small opportunity to encourage the child in their active involvement and its use in children with Cerebral Palsy is not recommended.
Therapeutic Interventions
Passive Stretching for athetoid cerebral palsy
- It is a manual application for spastic muscles to relieve sloppy tissue tightness.
- Manual stretching may increase the range of movements, decrease spasticity, or improve walking efficiency in children with spasticity.
- Stretch may be applied in a number of ways during neurological rehabilitation to attain different effects.
The types of stretching used include:
- Fast or Quick
- Prolonged
- Maintained
- When we look at the use of a stretch for facilitation, we employ a fast or quick stretch.
- The fast or quick stretch produces a relatively short-lived contraction of the agonist’s muscle and short-lived inhibition of the antagonist muscle which facilitates a muscle.
- It achieves its effect along stimulation of the muscle spindle primary endings which result in reflex facilitation of the muscle along the monosynaptic reflex arc.
- The presence of increased tone can ultimately first to joint contracture and changes in muscle length.
- When we look at the use of stretch to normalize tone and maintain soft tissue length we employ a steady, prolonged stretch to maintain or stop the loss of range of motion.
- While the effects are not wholly clear the prolonged stretch produces inhibition of muscle responses which may help in reducing hypertonus, for example, Bobath’s neuro-developmental technique, inhibitory splinting, and casting technique.
- It appears to have an influence on both the neural components of muscle, along the Golgi Tendon Organs and Muscle Spindles, and the structural components in the long term, along with the number and length of sarcomeres.
- Muscle Immobilised Shortened Position = Loss of Sarcomeres and Increased Stiffness related to enlargement in connective tissue.
- Muscle Immobilised Lengthened Position = Increase Sarcomeres.
Manual Stretching for athetoid cerebral palsy
- Prolonged physical stretch may be applied manually, using the effect of body weight and gravity, or mechanically, using machines or splints.
- Stretch should provide enough force to overcome hypertonicity and passively lengthen the muscle.
- Unlikely to provide enough stretch to cause a change in a joint that already has contracture.
Weight Bearing for athetoid cerebral palsy
- Weight-bearing has been reported to reduce contracture in the lower limb through the use of Tilt-tables, and standing frames via a prolonged stretch.
- Angles are key to making sure the knees remain extended during the prolonged stretch as the force exerted on the knee can be quite high.
- Certain research also challenges the assumption of the benefits of prolonged standing.
- Splints and casts are exterior devices “Splints and casts are external devices designed to apply, distribute or remove forces to or from the body in a controlled manner to perform one or both basic functions of control of body motion and modification or prevention in the shape of body tissue.”
- Splinting can be used to produce low-force, long-duration stretching although there is a deficiency of evidence to support this.
- A wide range of splints has been used to influence swelling, resting posture, spasticity, and active and passive Range Of Motion (ROM).
- A systematic review suggested that Lower Limb Serial Casting increased ankle dorsiflexion passive range of motion, reduced hypertonicity, and improved gait in children with Cerebral Palsy.
Splinting for athetoid cerebral palsy
- Serial casting is a usual technique that is used and is most effective in managing spasticity-related contracture.
- Serial casting is a specialized technique to give an increased range of joint motion.
- The process requires a joint or joints that are tight, which are immobilized with a semi-rigid, well-padded cast.
- Serial casting requires the repeated applications of casts, typically every one to two weeks as the range of motion is restored.
- The duration of the stretch to reduce both spasticities and prevent contracture is not clear from the research and requires further research to determine the most appropriate technique and duration to produce the required effect.
Static Weight-bearing Exercises for athetoid cerebral palsy
- Stimulation of antigravity muscle strength, the precaution of hip dislocation, reduction in spasticity, and improvements in bone mineral density, self-confidence, and motor function have all been achieved through the use of Static Weight-Bearing exercises like as Tilt-Table and Standing Frame.
Muscle Strengthening Exercises
- It aims to increase the power of fragile antagonist muscles and of the corresponding spastic agonists and to provide the functional benefits of strengthening in children with Cerebral palsy.
- It increases to power of weak muscles and strengthens muscles in cerebral palsy children.
Functional Exercises for Athetoid Cerebral Palsy
- Training related to specific functional activities combining aerobic and anaerobic capacity and strength training in ambulatory children has been shown to significantly increase overall physical fitness, the intensity of activities, and quality of life.
- Training programs on static bicycles or treadmills have been shown to be beneficial for gait and gross motor development yet have not shown to have any impact on spasticity or abnormal movement patterns.
- A study suggests the application of plyometric exercises to the physical rehabilitation programs of children with unilateral Cerebral palsy could achieve more significant improvement in muscle strength and walking performance.
Body Weight Supported Treadmill Training for Athetoid Cerebral Palsy
- Stepping movements from Reflex Stepping Reactions are normally present in newborns and infants, in front of the infant starts to bear weight, stand and walk.
- Body Weight Supported Treadmill Training, is achieved through supporting the child in a harness on the treadmill in an upright posture limiting overall weight-bearing, on a steady moving treadmill, and eliciting the stepping movements.
- Treadmill training consequently allows the development of stepping movements needed for ambulation.
- Studies using 3-4 sessions per week lasting for 3-4 months have shown an increase in the lower extremity movements and gait patterns in children with cerebral palsy.
Electrical Stimulation for athetoid cerebral palsy
- The goal of electrical stimulation is to improve muscle strength and motor function. Electrical stimulation is given by Transcutaneous Electrical Nerve Stimulation (TENS) Unit which is portable, non-invasive, and can be used in the home setting by parents or the patient.
- Neuromuscular Electrical Stimulation (NMES) requires the application of transcutaneous electrical current that results in muscle contraction.
- Neuromuscular Electrical Stimulation has been postulated to increase muscle strength by increasing the cross-sectional area of the muscle and by increasing the recruitment of type two muscle fibers.
- Functional Electrical Stimulation (FES) mention to the application of electrical stimulation during a given task or activity when a specific muscle is expected to be contracting.
- Patel (2005) has shown there is certain evidence to support the use and effectiveness of Neuromuscular Electrical Stimulation in children with Cerebral Palsy yet found that many of the studies are limited by confounding variables including concomitant use of other therapies, broad variation in methods of application, heterogeneity of subjects, difficulty in measuring functional outcomes and less of control subjects.
- Mintaze (2009) proposes that neuromuscular and threshold electrical stimulation as a modality in Cerebral Palsy is used for strengthening the quadriceps muscles in ambulant diplegic children with Cerebral Palsy, who have difficulty with specific resistive strength training.
Gait Training
- kids with cerebral palsy at physical therapy to increase walking.
- Gait training is a type of physical therapy that focuses specifically on increasing walking functions.
- Many individuals with cerebral palsy may walk with an abnormal gait due to spasticity in the legs. During gait training, a physical therapist may focus on improving walking speed or correcting walking form.
- Correcting abnormal gait patterns is required because the poor form can ultimately compromise function and potentially lead to the development of chronic pain.
- Gait training may involve the use of equipment like walkers, bodyweight supporting treadmills, and parallel bars to help individuals practice walking without losing stability.
- Additionally, a PT may recommend wearing orthotics like a leg brace to support correct musculoskeletal alignment and gently stretch spastic muscles.
- Gait training focuses on increasing the functions like:
- walking speed
- walking endurance
- gross motor function
- step length
Aquatic Therapy for athetoid cerebral palsy
- Aquatic therapy is a form of physical therapy that takes place in a pool.
- Being immersed in water allows individuals to feel weightless, which enables them to focus on developing their form without straining the joints.
- Additionally, moving against the resistance of water assists mildly in strengthening the muscles.
Aquatic therapy for cerebral palsy can involve different water-based exercises, including:
- Walking (or skipping, galloping, or running) in shallow or deep water
- Aquatic yoga
- Swimming
- Floating
- Motion exercises
- Resistance exercises
- Balance exercises
- Games
- Deep breathing exercises
- Stretching
Benefits of aquatic therapy for cerebral palsy involve improved:
- Gait
- Gross motor function
- Joint range of motion
- Cardiovascular endurance
- Posture
- Balance
- Spasticity reduction
- Circulation
Hippotherapy
- Gross Motor Function including Muscle tone, Range of Movement, Balance, Coordination, and Postural Control in Children with Cerebral palsy has been shown to improve with Hippotherapy – Therapeutic horseback riding which may decrease the degree of motor disability.
- Many none physical benefits may also be developed via enjoyment and providing a setting for increased social interaction, and cognitive and psychosocial development.
- Sharan et al (2005) have noted satisfactory results with Hippotherapy in Bangalore, especially the post-surgical rehabilitation.
- There is limited evidence available with two lower-quality trials on saddle riding on a horse that found no connecting-group differences in muscle symmetry or in any of the seven different outcome measures, excluding the sub-item of grasping.
Sensory Integration Training for Athetoid Cerebral Palsy
- Sensory integration therapy is based on the idea that certain kids experience “sensory overload” and are oversensitive to certain types of stimulation.
- When children have sensory overload, their brains have trouble processing or filtering lots of sensations at once.
- Meanwhile, other children are under-sensitive to certain kinds of stimulation.
- Children who are under-sensitive don’t process sensory messages quickly or efficiently.
- These children may notice disconnected from their environment.
- In either case, children with sensory integration issues scuffle to organize, understand, and respond to the information they take in from their surroundings.
- Sensory integration therapy reveals children to sensory stimulation in a structured, repetitive manner.
- The theory behind this treatment approach is that, over time, the brain will adapt and permit them to process and react to sensations more efficiently.
- In this concept, struggling in planning and organizing behavior are attributed to problems in processing sensory inputs within the Central nervous system, including vestibular, proprioceptive, tactile, visual, and auditory.
- Children with sensory integration dysfunction regularly use different sensory combination strategies.
- Treatment centers on the integration of neurological processing by facilitating the individual to process the type, quality, and intensity of sensation.
Games and Activities for Athetoid Cerebral Palsy
- When working with children, physical therapists may employ fun games and activities in addition to exercises to inspire the carryover of skills learned in therapy to a child’s daily life.
- This may include using obstacle courses, balance games, or even employing technology like Wii Fit.
- Ultimately, the key to increasing motor functions is to keep moving.
- Teaching children a fun, engaging activities that they can play at home can be an effective way to promote movement outside of physical therapy sessions and improve the carryover of skills and improvements.
- Arts and Crafts
- Adaptive Sports
- Board Games
- Karaoke(singing)
- Music Glove
- Photography
- Horseback Riding
Horseback riding is one of the best activities for kids with cerebral palsy because it encourages:
- Balance,
- Strength,
- Posture,
- Coordination,
- Range of motion.
- Swimming
- Swinging
- Hula Hooping
- Dance Party
Certain examples of songs with hand motions or dance moves include:
- Hokey Pokey,
- Head, Shoulders, Knees, and Toes,
- Hand Jive,
- Cha Cha Slide,
- Cupid Shuffle,
- Macarena.
- Hand-Clapping Games
The corresponding hand motions usually involve repetitive:
- Bending and straightening of the elbows,
- Accuracy to clap your partner’s hands,
- Wrist range of motion,
- Opening and closing of the hands.
Examples of hand-clapping games involve:
- Miss Mary Mack,
- Down by the Banks of the Hanky Panky,
- Slide,
- Lemonade,
- I Went to a Chinese Restaurant.
- Hot Lava
- This game will help your child control where they place their steps and encourage balance.
14. Darts
Playing with darts is a fun, challenging activity that can assist kids with cerebral palsy practice:
- Gripping smaller objects,
- Timing when to let go,
- Aiming,
- Bending and straightening their elbow,
- Wrist movements.
- Create a Secret Handshake
Task-oriented approach for athetoid cerebral palsy

- This treatment is established on the requirements of the child.
- Today the child is given the possibility to be further an active problem solver (instead of, as previously, a passive recipient of treatment) in the context of the day-to-day environment.
- The aim of this therapy for children with Cerebral palsy, as for most children with developmental disabilities, is to facilitate the child’s participation in everyday life situations, for example, to communicate with parents, siblings, and peers; to proceed from one place to another; to dress and undress; to eat, and to play.
- The choice of goals for therapy is supported by many factors: the child’s liking and the family’s preferences, the society and environment in which the family lives, and the child’s degree of disability.
- Consequently, it is important to integrate principles of motor learning into the treatment concept and adapt the principles to the prerequisites of each specific child.
- The regulated goals should be specific, measurable, attainable, relevant, and timed (SMART).
Conductive Exercise
- Conductive education (CE) is a combined educational and task-oriented approach for children with Cerebral palsy.
- Specially instructed ‘conductors’ give education to homogeneous groups of children with motor disorders.
- These proceeds have their origins in learning theory.
- The conductor who is trained in all aspects of motor and cognitive development structures the activities, especially the self-care activities.
- The emphasis of interference is on independence in attaining goals rather than on the quality of movement.
Bimanual Training
- Bimanual Training (BIT) provides bimanual training activities, which focus on increasing the coordination of both arms using structured tasks in bimanual play and functional activities with intensive practice.
- Recently has an exhaustive bimanual training program, the hand-arm bimanual exhaustive training (HABIT) been published to substantiate its effectiveness.
- This approach is founded on motor learning theory (practice specificity, types of practice, and feedback), neuroplasticity (i.e., the potential of the brain to change by repetition, increasing movement complexity, motivation, and reward), and focuses on the same use of both arms in bimanual tasks.
- Intensive Bimanual training (e.g., HABIT), was developed with the recognition that increased functional independence in the child’s environment needs the combined use of both hands.
- It as well as focuses on improving coordination of the two hands using structured task practice embedded in bimanual play and functional activities.
- Hand-arm bimanual intensive therapy including lower extremities (HABIT-ILE) integrates upper and lower bilateral extremity training.
- Usually used bilateral lower extremity tasks are ball sitting, standing, balance board standing, virtual reality (Wii-fit, Kinect), walking/running, jumping, cycling, and making scooters.
- Bimanual activities that require trunk and lower extremities postural adaptations are performed at a table of appropriate height (50% of the time) on unstable supports: sitting on fitness balls or standing on balance boards.
- Moreover, 30% of the time is devoted to activities of daily living where standing and/or walking is required (dressing, brushing teeth, doing one’s hair, transporting objects such as a tray, and household chores like as sweeping and washing dishes).
- Finally, the remaining time (20%) is spent in gross motor physical activities/play, like bowling, ball playing, jumping rope, street hockey, use of Wii-fit, balance bike (without pedals), scooter use, and wall climbing.
- These are performed in standing, walking, and running (or jumping) with the lower extremities and simultaneously involve bimanual coordination.
- These activities are graded toward more demanding tasks for the lower extremities.
Robot-assistive therapy for athetoid cerebral palsy
- Robot-assisted therapy (RAT) is conducted using robotic devices that allow the patients to perform specific limb movements.
- The foremost interest in using robots is to allow the patients to achieve a large amount of movement in a limited time.
- Additionally, the attractive human-machine interface has the capacity to motivate the child to perform his or her therapy via playful games, like car races, or to perform exercises that mimic activities of daily living.
- Moreover, robotic devices permit the patient to receive visual, auditory, or sensory feedback.
- A device specifically developed for locomotion training is the Lokomat (Hocoma, CH), made of 2 active orthoses, a weight-bearing system, and a treadmill.
- This robotic rehabilitation has been proposed to increase walking and physical fitness.
Virtual reality for athetoid cerebral palsy
- Virtual reality has been defined as the use of interactive simulations created with computers to perform users in virtual environments that appear, sound, and feel the same as real-world objects and events.
- Virtual reality can improve the patient’s motivation and achievement in activities of daily living.
- Preliminary data suggest that this type of therapy also improves motor function in the upper and lower extremities that are caused by Cerebral palsy.
State of the Evidence
- Novak et al. (2013) have developed a chart founded on their Systematic Review, which looked at the State of the Evidence in relation to Interventions for the management of children with Cerebral Palsy, to help with comparative clinical decision-making amongst intervention options for the same desired outcome.
- They charted the interventions using bubble charts, with the size of the circle correlated to the volume of published evidence.
- The circle size was calculated using;
The number of published papers on the topic:
- Entire score for the level of evidence (calculated by reverse coding of the Oxford Levels of Evidence, for example, expert opinion=1, randomized controlled trial [RCT]=5).
- The location of the circle on the Y-Axis of the graph correlates to the GRADE System Rating.
- The Colour of the circle corresponds to the Evidence Alert System.
Speech and Language Therapy for athetoid cerebral palsy:
- Individuals with Cerebral Palsy frequently have difficulties with their speech and swallowing. Difficulties in written and non-verbal communication can too be experienced.
Our specialist speech and language therapists can help with:
- Training for family and carers on how to communicate with the person with dysphasia.
- Advice and management with different communication aids.
- Treatment in the middle or in your own home.
- Assistance with a written communication as well as adaptive equipment.
Neuropsychology for athetoid cerebral palsy:
- Cerebral Palsy is a long-lasting condition and affects people of all ages.
- Coming to terms with the symptoms and mislaying of independence at any age is a challenge.
Our clinical neuropsychologists can help to provide:
- Detailed assessment of a client’s functioning in specific to their cognition, behavior, and emotional state.
- Providing advice, consultation, teaching, and supervision to other professionals also family and carers.
- Management and guidance for anxiety and changes in mood.
Orthotics for athetoid cerebral palsy
- Orthotics may be an everyday requirement that often needs re-adjusting as the person grows.
- Our specialist orthodontist can help by designing, fitting, and altering orthoses to satisfactory complement your treatment and rehabilitation.
These include:
- Orthotics to fend off foot drops and aid walking,
- Night and day resting splints to prevent alignment and prevent contractures,
- Insoles to make better alignment, proprioception, and gait,
- Variation to shoes to assist with leg length discrepancies, alignment, and improved mobility.