TAPING TECHNIQUE FOR ACL INJURY
Table of Contents
Introduction:
Tapping is the most effective technique for anterior cruciate ligament injury. it is the most popular technique. also called kinesiology tape or kinesiology therapeutic tape, is an elastic cotton strip with an acrylic adhesive that is purported to ease pain and disability from athletic injuries and a variety of other physical disorders. Taping your knee can help stabilize it when you’re active and can give relief from pain.
Kinesiological taping is a rehabilitative cum protective use of stretchable kinesiological tapes to provide:
- reduction in knee pain while acl injured
- enhancing performance of affected knee
- preventing further injuries to the knee
- support to the knee joint
- repositioning of the structure of the knee
- facial and ligamentous correction of the knee.
- It facilitate the healing process while providing full ROM with support to the joints suppotive structure as well as mobilization effects. An anterior cruciate ligament injury occurs when the anterior cruciate ligament (ACL) is either stretched, partially torn, or completely torn.
- The most common injury is a complete tear. Symptoms include pain, an audible cracking sound during injury, instability of the knee, and joint swelling. Swelling generally appears within a couple of hours.
- In approximately 50% of cases, other structures of the knee such as surrounding ligaments, cartilage, or meniscus are damaged. The underlying mechanism often involves a rapid change in direction, sudden stop, landing after a jump, or direct contact with the knee.
- It is more common in athletes, particularly those who participate in alpine skiing, football (soccer), American football, or basketball. Both contact and non-contact injuries can occur, although non-contact tears and ruptures are most common.
- It appears that females tend to have a higher incidence rate of ACL injury than males, that being between 2.4 and 9.7 times higher in female athletes competing in similar activities.
Relevant anatomy:

- The ACL could be a band of dense animal tissue that courses from the leg bone to the leg bone. it’s thought of as a key structure within the ginglymoid joint because it resists anterior leg bone translation and motion masses.
- The ACL arises from the posteromedial corner of the medial side of the lateral leg bone appendage within the intercondylar notch and inserted anterior to the intercondyloid eminence of the leg bone, mixing with the anterior horn of the medial cartilage.
- The ACL courses anteriorly, medially, and distally across the joint because it passes from the leg bone to the leg bone.
- As it does, it activates itself during a slight outward (lateral) spiral. There area unit 2 parts of the ACL, the smaller anteromedial bundle (AMB) and also the larger posterolateral bundle (PLB), named per wherever the bundles are inserted into the leg bone upland.
- once the knee is extended the PLB is tight and also the AMB is moderately lax. However, because the knee is flexed, the leg bone attachment of the ACL assumes an additional horizontal orientation, inflicting the AMB to tighten and also the PLB to loosen and therefore leave the AMB because of the restraint to the anterior leg bone load.
Function of ACL:
- Primary restraints to anterior tibial displacement: counting for 85% of the resistance to anterior drawer test, when the knee is kept at 90 degrees of flexion.
- Secondary restraints to tibial rotation & varus: valgus angulation at full knee extension.
- Proprioceptive function: the presence of mechanoreceptors in the ligaments.
Causes of ACL injury:
- Ligaments are strong bands of tissue that connect one bone to another. The ACL, one of two ligaments that cross in the middle of the knee, connects your thighbone to your shinbone and helps stabilize your knee joint.
- ACL injuries often happen during sports and fitness activities that can put stress on the knee:
- Suddenly slowing down and changing direction (cutting)
- Pivoting with your foot firmly planted
- Landing awkwardly from a jump
- Stopping suddenly
- Receiving a direct blow to the knee or having a collision, such as a football tackle
- When the ligament is damaged, there is usually a partial or complete tear of the tissue. A mild injury may stretch the ligament but leave it intact.
Symptoms of ACL injury:
- The primary sign of an ACL injury is a popping noise. This is often combined with pain and swelling.
- You could experience grinding feelings in your bones or kneecap. Another sign is not being able to put weight on your leg.
- People with a mild ACL injury might feel like their knee is unstable, or like it might “give out” when they are using it.
Risk factors of ACL injury:
- Risk factors for ACL injuries include environmental factors (e.g. high level of friction between shoes and the playing surface) and anatomical factors (e.g. narrow femoral intercondylar notch). The injury is characterized by joint instability, which is associated with both acute dysfunction and long-term degenerative changes such as osteoarthritis and meniscal damage.[19] Knee instability leads to decreased activity, which can lead to poor knee-related quality of life.
- The risk factors for ACL injury have been considered as either internal or external to an individual. External risk factors include the type of competition, footwear and surface, and environmental conditions. Internal risk factors include anatomical, hormonal, and neuromuscular risk factors.
- external risk factors :
Competition in games versus practice
Footwear and playing surface
Protective equipment
Meteorological conditions - Internal Risk Factors
Anatomical risk factors: Abnormal posture, and lower extremity alignment contributing to increased ACL strain values
Grades of ACL injury:
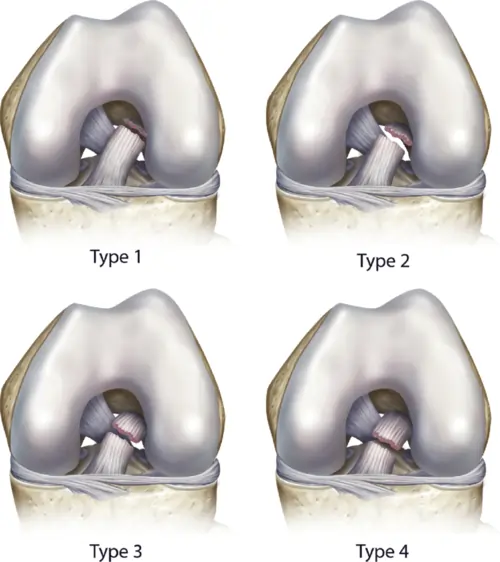
- Grade one Sprains: The ligament is gently broken in an exceedingly Grade one Sprain. it’s been slightly stretched, however continues to be able to facilitate keeping the hinge joint stable. There is very little swelling and tenderness. There is an associate degree firm finish feel. no increase in neglect of joint.
- Grade a pair of Sprains: A Grade a pair of Sprain stretches the ligament to the purpose wherever it becomes loose. typically|this can be} often spoken as a partial tear of the ligament. The fibers of the ligament square measure partly torn or incompletely torn with hemorrhage.
- There is a touch tenderness and moderate swelling with some loss of operate. The joint might feel unstable or provide out throughout the activity. Increased anterior translation nevertheless there’s still a firm finish purpose. Painful and pain increase with Lachman’s and anterior drawer stress tests.
- Grade three Sprains: this kind of sprain is most ordinarily spoken as an entire tear of the ligament. The ligament has been split into 2 items, and also the hinge joint is unstable.
- Partial tears of the anterior symmetrical ligament square measure rare most ACL injuries square measure complete or close to complete tears. There could also be a touch of swelling or tons of swelling. The ligament cannot management knee movements. The knee feels unstable or offers out at certain times. There is additionally move instability as indicated by a positive pivot shift check.
- No end purpose is obvious. Haemarthrosis happens within 1-2 hours. associate degree ACL avulsion happens once the ACL is torn aloof from either the thighbone or the shinbone. this kind of injury is additional common in youngsters than adults. The term anterior symmetrical deficient knee refers to a grade III sprain during which there’s an entire tear of the ACL. it’s typically accepted that a torn ACL won’t heal.
- Special test for acl injury
Special test for ACL injury:
- Lachman test :
procedure: patient supine with knee flexed 0-30 degrees. stabilize femur.apply posteroanterior force to tibia.
positive sign: soft end feel or excessive movement. - Anterior drawer test :
procedure: patient supine with hips flexed to 45 degrees and knee flexed to 90 degrees. stabilize foot. apply posteroanterior force to tibia.
positive sign: tibia moves more than 6 mm on the femur. - Slocum test :
procedure: patient supine with hips flexed to 45 degree and knee flexed to 90 degree. place the foot in a 15-degree lateral rotation and stabilize. apply posteroanterior force to tibia .
positive sign: excessive movement on the medial side when compared with other knees.
Methods for tape recording Your Knee:
- A technique used: ligament technique.
- Structure: anterior cruciate ligament.
- Attachments: It connects the lateral epicondyle of the femur with the head of the fibula.it attaches superiorly to the lateral wall of the intercondylar notch at its posterior aspect.
- inferiorly it is attached to an oval-shaped area, the anterior aspect of the tibial plateau between the tibial eminences.
- Function: prevent hyperextension and excessive internal rotation. the anterior cruciate ligament limits the anterior movement of the tibia relative to the femur in all positions of joint movement.
- Subject position: The subject is supine lying in a relaxed comfortable position.
- Therapist position: The therapist standing at the foot end of the subject.
- Strip: I strip is used.
Procedure :

- Follow the basic steps for ligament taping.
- Measuring the tape: The tape strip size depends on the physique of the subject. the strip should be 2cm more in length than the application area.
- Select the required strip design, generally ”I”strip is used.
- The corners of the tapes are rounded off.
- Application of tape: The backing paper is torn off from the center, the tape is stretched to 75-100% of its length, and the center of the tape is applied anteriorly just below the inferior pole of the patella while the subject is moving the knee into flexion, and both the ends are attached without any stretch. The application is repeated with 2 strips if needed. The first strip is always parallel to the ligament attachment. At the end of the application rub the tape until the warmth is felt, this is necessary to activate the glue.
How to remove KT:
- So presently you’ve got your tape on and you’ve gotten that additional support throughout your chosen sporting activity, it’s time to need it off, so enable the United States to ease the tactic of removing physiology tape for you. the foremost effective tip we are going to provide once it involves removing your physiology tape is to peel the skin from the tape, not the tape from the skin.
- But in terms of the actual methodology, 1st ensure you’re removing the tape in an equivalent direction as a result of the expansion of the hair below it, and despite what you’re doing don’t rip the tape off kind of a plaster!
- Start slowly, folding the corners of the sting back bit by bit, guaranteeing that you’re birth the removed tape on the rear of the applied tape, as opposition propulsion the tape on top of and aloof from your arm.
- As you’re scraping the tape, hold your skin down beside your completely different hand and either regulator it or
- pull it gently among the opposite means of the tape. This helps the skin and so the tape to separate heaps expeditiously but with no discomfort.
- If the tape has been applied over a furred region of the body, it helps to maneuver on the tape as you are peeling it off, as a result of the pressure helps avoid a lot of pain.
- It’s knowing have shaved the realm before applying the tape but, as this isn’t frequently smart, taking this precaution square
- measure reaching to be necessary to some.
- want a bit of additional assistance? Apply oil directly onto the tape, rub it in, and wait around 10 to twenty minutes before removing it slowly. This will facilitate reducing the viscousness of the tape and build it easier to induce obviate.