Lumbar traction
Table of Contents
What Is Lumbar Traction?
Lumbar traction is a physical therapy treatment often combined with exercise, that is sometimes used for low back pain or sciatica. Lumbar (low back) traction helps to split the spaces between the vertebrae, the bones that make up the spine. The process stretches the space between the vertebrae in the lower spine, helping to ease lower back pain. Theoretically, separating these bones slightly can alleviate pain and increase mobility by relieving pressure on pinched nerves like the sciatic nerve.
Clinically Relevant Anatomy
The concave lumbar curvature in the lower back is formed by the five separate vertebrae of the lumbar spine, which are numbered L1 to L5. The lumbar vertebrae make up the region of the spine that is inferior to the thoracic vertebrae in the thorax and superior to the sacrum and coccyx in the pelvis. It is located along the body’s midline in the lumbar (lower back) region. All of the weight of the upper body is carried by these vertebrae, which also give the trunk region flexibility and movement.
An intervertebral disk of hard fibrocartilage with a jelly-like center connects each vertebra to its neighboring vertebra. The outer layer of the intervertebral disk, which is called the annulus fibrosis, holds the vertebrae together and provides strength and flexibility to the back during movement. The jelly-like nucleus pulposus serves as a shock absorber, to withstand the pressure and strain on the lower back,
The lumbar vertebrae are probably the biggest and heaviest vertebrae in the spine, second in size just to the sacrum. The vertebral body, a cylinder-shaped piece of bone, supports the majority of the weight of the body on the lumbar vertebrae. The body connects to the arch, a thin bone ring, posteriorly. The body is connected to the bony processes on the posterior of the vertebra by the arch, which surrounds the hollow vertebral foramen. The spinal cord, cauda equina, and meninges have room to move through the lower back through the vertebral foramen, a large triangular opening in the middle of the vertebrae.
Extending from the vertebral arch are several bony processes that are concerned with muscle attachment and movement of the lower back. The spinous cycle stretches out from the back finish of the curve as a flimsy square shape of a bone. The muscles of the back and pelvis, like the psoas major and interspinales, come together at this point. The short, triangular transverse processes are located on each vertebra’s left and right lateral sides. The rotatores and multifidus muscles, which extend and rotate the trunk, use the transverse processes as important connection points.
The lumbar vertebrae, in contrast to the cervical vertebrae in the neck, lack facets on either side of the body and the transverse foramina in the transverse processes. In contrast to the L1-4 vertebrae, the L5 vertebrae are significantly larger on their front side than on their back. On the other hand, it has a wider, four-sided shape, a rough edge, and a deep notch on its spinous process, which is smaller than that of the other lumbar vertebrae.
Types of Lumbar Traction:
The most common types of lumbar traction, according to the literature, are:
Continuous Traction: This type of traction utilizes low weights for long periods (several hours at a time). Because of the long duration, only a small amount of weight needs to be used. It is a common misconception that this kind of traction is not effective enough to separate the structures of the spine. To put it another way, the patient is unable to bear weights that would cause the vertebrae to separate for that amount of time.
Sustained Traction: For brief periods (ranging from a few minutes to one hour), this type of traction applies heavier weights consistently. Sustained traction is sometimes directed to as static traction.
Intermittent Mechanical Traction: Intermittent traction is equal to sustained traction in intensity and duration but operates a mechanical unit to alternately apply and release the traction force at preset breaks
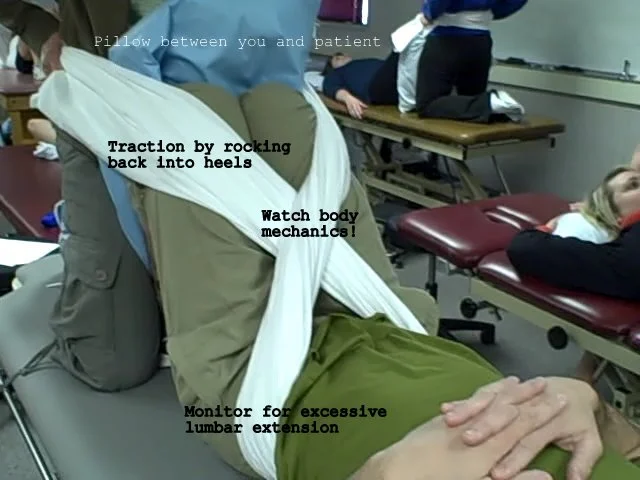
Manual Traction – Manual traction is applied as the clinician’s hands and/or a strap is used to pull on the patient’s legs. It is typically applied for a few seconds, but it can also be applied abruptly and quickly.
Autotraction: A specialized table with two sections that can be tilted and rotated independently is used in autotraction. The patient delivers the traction force by drawing with the arms and/or pushing with the feet.
Positional Traction: Positional traction is a type of traction in which the patient is placed in a variety of positions and supported by pillows, blocks, or sandbags to produce a longitudinal pull on the spinal structures. It typically consolidates horizontal bowing and is simply impacted aside from the spinal fragment
Gravity lumbar traction: While the treatment table is tilted to the vertical position, a chest harness is used to secure the patient. The traction force is generated by the patient’s body weight in the lower half of the body.
Mechanism:
The potential clinical benefit of traction therapy has been the subject of several hypotheses. The nucleus pulpous’s position in relation to the posterior annulus fibrosis or the disc-nerve interface should be altered by distracting the motion segment. Studies of the lumbar spine’s kinematics during traction therapies may be the source of these effects. As well as isolating the vertebrae, foothold has been displayed to diminish core pulposus pressure and extend the foraminal region. In any case, it is impossible that mechanical changes seen in an inclined position will be supported after a patient proceeds with an upstanding, weight-bearing stance. The traction’s effect on the motion segment’s mechanobiology or neural tissues is more likely to account for any long-term clinical response. The fact that not all traction therapies work the same way on the spine and that studies on animals have shown that the disc’s mechanobiology is sensitive to the amount, frequency, and duration of loading adds complexity to the situation.
It’s possible that some types of traction encourage tissue degradation while others help the discs or joints heal. Even though these variables haven’t been looked at in a systematic way, even in animal models, what we know about disc mechanobiology suggests that not all traction therapies are created equal. On the off chance that diverting the spine can impact plate and joint mechanobiology, various methods of footing might bring about various clinical outcomes. The possibility of distinct effects based on force and time parameters has not been taken into account in the majority of lumbar traction therapy systematic reviews. Patients with a mix of clinical presentations, such as leg-dominant LBP, back-dominant LBP, or both, have typically participated in traction trials. In any case, a patient with just prevailing LBP and no radiculopathy is probable encountering torment from a sclerotome source, for example, feature joints or plate, though sciatic torment, regardless of whether brought about by circle herniation, might prevail of brain beginning. Although there is insufficient evidence to support this hypothesis, it is reasonable to speculate that traction therapies may affect these conditions in different ways.
Interruption control and positional interruption are precisely not the same as customary footing (discontinuous or supported). These treatments attempt to focus forces in a smaller area rather than allowing them to spread throughout the lumbar tissues. For instance, AT lets the patient focus the force by distracting themselves in the position that helps them feel the least pain. The majority of chiropractors and physical therapists use distraction manipulation, which is performed on treatment tables that allow the operator to select the moment-to-moment vector and timing of the distractive force.
Indications:
Spinal traction has been utilized for the treatment of the conditions given below:
- Spinal nerve root impingement:
- Herniated disc
- Ligament encroachment
- Narrowing of the intervertebral foramen
- Osteophyte encroachment
- Spinal nerve root swelling
- Spondylolisthesis.
- Degenerative joint disease
- Extrinsic muscle spasm and muscle guarding
- Discogenic pain
- Joint pain
- Compression fracture
- Joint hypomobility
Contraindications:
Traction to the lumbar spine is contraindicated in many of the conditions. The physical therapist must take a proper medical history before prescribing traction for back pain.
- Acute strains
- Sprains
- Inflammation
- Respiratory problem
- Claustrophobia
- Osteoporosis
- Infection
- Tumor
- Rheumatoid arthritis
- Pregnancy
- Cardiovascular disease
- Hernia
- Cauda Equina Syndrome
- Neoplasms
- Pott’s Disease
- All inflammatory diseases of the vertebrae
- Cardiac or circulatory disease
- Severe respiratory problems
- Post-operative patients with 3 months of back surgery
- Vertebral fracture within 6 months of the initial injury
- Fusion with internal fixation
How much weight is safe and effective?
Lumbar traction weight calculation:
The weight, height, and build of each person who comes to you will vary. The weight that works for one person might not be right for another. A therapist needs to calculate the weight of each and every different person.
The weight of pull for lumbar traction should be 1/3 of the body’s weight, according to a general rule. ITen people with positive unilateral SLR tests below 45′ and subjective complaints of low back pain or radicular symptoms. As indicated by research, footing utilizing somewhere in the range of 30 and 60 percent of one’s body weight resulted in significant improvements in lower extremity mobility.
Note: The pull for neck or cervical traction is one-seventh (1/7th) of the body’s weight.
For instance, if a person weighs 65 kilograms, the force of pull would be approximately 21.5 kilograms or 1/3 of 60 kilograms. Therefore, 25 kg would be ideal in this circumstance.
How to Prepare for Lumbar Traction?
The traction is applied by using motorized devices that utilize pelvic and thoracic belts. These belts are applied directly in contact with the patient’s skin and not over the clothing. Both belts should be tight sufficient to prevent slipping.
Placement Of Thoracic Belt:
The upper limit at which the traction force is required is aligned with the lower edge.
The upper edge is roughly aligned with the xiphoid just below the thorax’s greatest diameter.
Placement Of Pelvic Belt:
Its prevalent edge lines up with as far as possible at which foothold force is wanted.
Position in the supine position, just above the iliac crest.
Prone position-superior to the superior edge of the sacrum.
The prone position is more useful when a person has moderate to severe pain or has muscle guarding.
The machine has got a fixed and mobile part and a lower body that rests on the mobile unit gets separated from the fixed unit as the tactile force is applied. It is found that with the hips flexed 70 and an angle of pull of 18 is created which provides the greatest vertebral separation.
Positioning:
A supine position is typically chosen due to the separation of posterior components and the localization of traction force to the upper lumbar and thoracic segments.
Weight used in lumbar traction:
A human body lying on a couch or mattress has a coefficient of friction of 0.5. To move the patient’s body horizontally, a force equal to % of the patient’s body weight is required. A force equal to % x 0.5 = 1/4 of the body weight is lost to overcome friction as half of the body weight lies beneath L-3. As a result, if conventional bed traction methods are used, only a weight that is between 1/4 and 1/2 of the patient’s body weight can effectively exert a traction force. Any less than 1/4 of the patient’s body weight will not be enough to cause the patient to slide to the foot of the bed.
The quantity of force alone does not define the effectiveness of the traction treatment. The comfort of the patient is of tremendous importance. If the patient is not able to relax with the treatment, it will likely be ineffective. Some evidence demonstrates that a narrowing of the intervertebral spaces can occur with the inability to relax. For the patient to relax, the treatment must not aggravate his/her condition, and the patient must feel secure and well-supported. It may be useful to administer modality treatments before the traction application. Such therapy as ice, heat, ultrasound, or massage is often effective. The use of a heavy-duty nonslip traction harness is necessary. If the patient does not feel safe, he or she will almost certainly remain tense during the treatment.
This harness which is used in traction is lined with a vinyl material that causes it to adhere to the patient’s skin, thus stopping the slipping that is common with cotton-lined belts. Both the pelvic and thoracic pads should be placed subsequent to the patient’s skin. It will be more likely for the clothing to allow slippage if it is left under the harness. Attire may likewise take a portion of the footing force on the off chance that it is bound firmly under the two belts. The thighs of patients might give them better support and help them relax. It discusses how to precisely concentrate the tractive force by varying the patient’s leg position or lumbar flexion. He states attraction occurs in the lower lumbar region when there is little or no lumbar flexion. When the knees are flexed against the chest, the tractive force is directed to the upper lumbar and lower thoracic regions.
Lumbar traction kit at home:
A lumbar traction kit is used to treat low back pain at home.
The lumbar traction kit consists of:
- Backboard
- Straps
- Weights
- Traction pully
- Pelvic belt: It bears the pelvic region firmly without any discomfort and the two side belts provide traction in the parallel direction of the legs.
- Spreader bar with hook
- Spreader bar: It maintains the traction belt and controls the pulley rope flexibly for movement.
- 3-meter long cord
- Water bag: It is made of durable material to keep the required weight to perform traction.
The direction of use:
- Wrap the traction belt around the pelvic region and fasten it with velcro.
- Connect the belt to the traction pulley via the spreader bar with the suggested weight on the other side.
Many people also use these kits to stretch the lower back muscle.
There are various brands that sell it online:
- Tynor lumbar traction kit: Its superior design offers long-lasting performance and accurate focus of the traction force. it is an ideal solution for achieving desired results. It will help in getting recovery from neck or back pain. The cost of this kit ranges from Rs 1500-6000.
- Flamingo Lumbar traction kit: This kit is also for orthopedic care. It is not only a premium quality product but also offers an unbeatable solution for those who are suffering from the orthopedic problem. More effective relief can be achieved quickly and conveniently without any discomfort and pain. Its price ranges from Rs 1200-4500.
- Vissco traction kit: It is a trustworthy brand in a traction kit. It offers the best in terms of quality and performance. Lumbar traction kit price ranges from Rs 1000-4000.
Benefits of lumbar traction kit:
- The range of motion and mobility can be improved with the help of a lumbar traction kit.
- A lumbar traction kit can reduce the pressure on the pinched nerve.
- It improves the flexibility of muscles.
- It is one of the most efficient drug-free ways to relieve pain.
- Traction therapy has proven a record of reducing stress in the affected area.
Summary:
Lumbar traction can be a viable technique for solutions for various normal musculoskeletal problems. The administration of effective treatment is not as straightforward as it may appear. There are numerous interpretations of the technique, some of which have questionable value. The physical therapist who intends to treat patients with spinal traction should get comfortable with the best procedures, and their application. Last but not least, the importance of the musculoskeletal evaluation cannot be overstated. The treatment plan will have very little chance of being successful if the information gathered during the evaluation is incorrect.
FAQs:
Does walking reduce disc bulge?
Generally speaking, as long as they’re performed correctly exercise. Core and back exercises are helpful for bulging discs, as are activities like walking, elliptical exercise, swimming, and riding a stationary or regular bike.
How long should you do lumbar traction?
The typical protocol for traction is the use of a force equal to 50% of the patient’s body weight and the use of an intermittent force pattern of 20 to 30 seconds on and 10 to 15 seconds off, for a total time of 15 minutes.
Is lumbar traction safe?
Traction is not at risk in the long run. During or after treatment, some side effects may occur. After traction, many people experience muscle spasms, and some experience pain in the treated area.
Is traction good for slip discs?
In conclusion, lumbar traction improves the symptoms and clinical findings of lumbar disc herniation patients and reduces the size of the measured CT herniated disc material.
Can traction cause nerve damage?
Although halo-suspension traction or halo-wheelchair traction may be slightly rigid, so, injury to the hypoglossal nerve can be produced with traction overreaching 40% of body weight.