Kinesio taping technique for Facial Palsy:
Table of Contents
Introduction:
Kinesio taping technique for Facial Palsy is used to correct facial deviation and enhancing overall treatment program. Gradually it is increasingly used in the rehabilitation of peripheral facial palsy. kinesio taping is used to maintain functional position of facial muscle that helps on peripheral facial palsy and the improvement of functions of face muscles.
its further support to the involved area of face. Now a days this is most effective and supportive treatment for facial palsy .It is give static as well as dynemic support to the face.
kinesio taping give dynamic support to the involved area while typical taping give static support to the involved area of treatment.
Bell’s palsy, also known as acute peripheral facial palsy of unknown cause, can occur at any age.
The exact cause is unknown. It’s believed to be the result of swelling and inflammation of the nerve that controls the muscles on one side of your face. Or it might be a reaction that occurs after a viral infection.
The symptoms of facial palsy include sudden weakness in your facial muscles. In most cases, the weakness is temporary and significantly improves over weeks. The weakness makes half of your face appear to droop. Your smile is one-sided, and your eye on that side resists closing.
Kinesiological tapping could be a rehabilitative cum protecting use of elastic kinesiological tapes to supply :
- kinesio taping facilitate facial muscle contraction
- reduction in face pain
- enhancing performance of affected face area
- repositioning of structure of face
- facial and ligamentous correction of the face.
- improve sensory inputs
- improve blood flow
- improve lymphatic drainage
Bell’s palsy causes temporary paralysis, or palsy, of facial muscles.Facial palsy is caused by damage to the facial nerve (i.e. cranial nerve VII) that supplies the muscles of the face. It can be categorised into two types based on the location of the casual pathology:
Central facial palsy : Due to damage above the facial nucleus.
Peripheral facial palsy : Due to damage at or below the facial nucleus.
Bell’s palsy is a common cranial mononeuropathy. It affects males and females equally, and has a slightly higher incidence in mid and later life, but certainly occurs across all age ranges.
The facial muscles are innervated peripherally (infranuclear innervation) by the ipsilateral 7th cranial nerve and centrally (supranuclear innervation) by the contralateral cerebral cortex. Central innervation tends to be bilateral for the upper face (eg, forehead muscles) and unilateral for the lower face.
As a result, both central and peripheral lesions tend to paralyze the lower face. However, peripheral lesions (facial nerve palsy) tend to affect the upper face more than central lesions (eg, stroke) do. Many people fear they are having a stroke, but if the weakness or paralysis only affects the face, it is more likely to be Bell’s palsy.
Anatomy related to facial palsy:
- The human facial nerve is the seventh cranial nerve (CNVII) and comprises motor, sensory and parasympathetic components.
- Its function is responsible for voluntary and mimetic facial movement, taste to the anterior two-thirds of the tongue, and control of exocrine gland and lacrimal gland secretions.
- The facial nerve receives axons from the superior part of the solitary nucleus and superior salivary nucleus that form the nervous intermedius component (sensory and parasympathetic axons) and motor efferent fibres from the facial nucleus, which receives synaptic input from the contralateral motor area for all facial movements except the forehead, which has bicortical input.
- The path of the facial nerve has intracranial, intratemporal and extratemporal elements.
- Its intracranial course runs from the pontomedullary angle to the internal acoustic meatus where it is accompanied by the vestibulocochlear nerve (CNVIII).
- The intratemporal course of the facial nerve is long and tortuous. During its intratemporal course, the nerve encounters the geniculate ganglion and gives rise to the superior petrosal nerve, the nerve to stapedius and chorda tympani nerve branches, before exiting the skull base through the styloid foramen.
- The extratemporal facial nerve courses through the substance of parotid gland dividing it into deep and superficial lobes. It gives off the posterior auricular nerve and nerve to the posterior belly of digastric before dividing into its terminal facial branches.
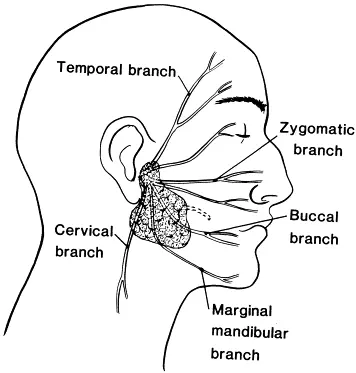
- There is significant variation in the branching pattern of the terminal facial branches, which are historically conceptualised into temporal, zygomatic, buccal, marginal mandibular and cervical branches.
- These terminal motor branches are responsible for all facial expression and functional tasks such as eye and mouth closure and nasal patency during inspiration.
- Throughout its course, the facial nerve forms multiple communications between its own branches and with adjacent cranial nerves.
Symptoms of facial palsy:
- The most noticeable sign is weakness and drooping on one side of your face. You’ll find it hard to close your eye on that side or make facial expressions like smiling. Your face may even be completely paralyzed on that side. It’s rare, but Bell’s palsy can sometimes affect the nerves in both sides of your face.
- Drool
- Feel pain in your jaw or behind your ear on the side that’s affected. Some people notice pain behind their ear 1 or 2 days before any weakness.
- Have a headache
- Have less sense of taste
- Have dry eyes and mouth
- Hear ringing in your ears (tinnitus)
- Be more sensitive to sound on the side that’s affected. Sounds seem much louder than normal in the days before you see any other symptoms.
- Find it hard to talk
- Have trouble eating and drinking
- Once they happen, symptoms usually get better over the next 3 weeks or so. Most people — up to 80% — have no symptoms at all within 3 to 6 months. Some people who get Bell’s palsy have a longer recovery period. In rare cases, they may have some permanent symptoms.
Causes of facial palsy:
Although the exact reason Bell’s palsy occurs isn’t clear, it’s often related to having a viral infection. Viruses that have been linked to Bell’s palsy include viruses that cause :
- Upper motor neurone causes:
- Stroke
- Intracranial tumour
- Multiple sclerosis
- Syphilis
- HIV
- Vasculitides
- Haemorrhage
- Cold sores and genital herpes (herpes simplex)
- Chickenpox and shingles (herpes zoster)
- Infectious mononucleosis (Epstein-Barr)
- Cytomegalovirus infections
- Respiratory illnesses (adenovirus)
- German measles (rubella)
- Mumps (mumps virus)
- Flu (influenza B)
- Hand-foot-and-mouth disease (coxsackievirus)
- The nerve that controls your facial muscles passes through a narrow corridor of bone on its way to your face. In Bell’s palsy, that nerve becomes inflamed and swollen — usually related to a viral infection. Besides facial muscles, the nerve affects tears, saliva, taste and a small bone in the middle of your ear.
Risk factors of facial palsy:
- Diabetes
- Pregnancy
- Potentially due to hypercoagulability, increased blood pressure and fluid load,
- viral infections and suppressed immunity
- Ear infection
- Upper respiratory tract infection
- Obesity
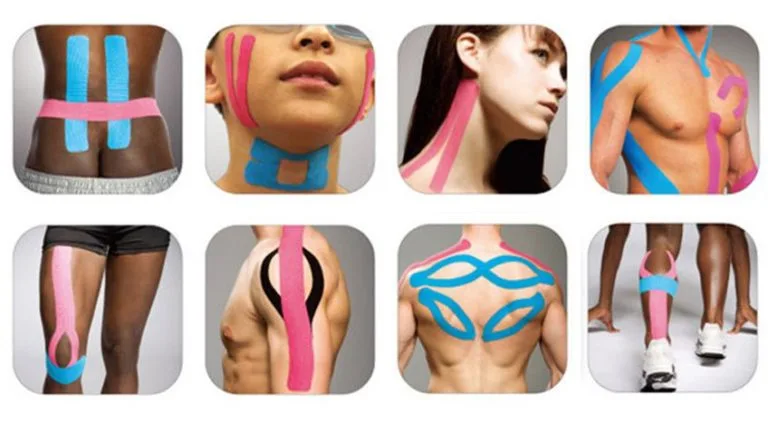
Kinesio taping for facial palsy:
Developed By Dr. Kenzo Kase in 1979. The Kinesio Taping Method is the definitive rehabilitative taping system of knowledge, is designed to facilitate the body’s natural healing process while providing support and stability to muscles and joints without restricting the body’s range of motion, as well as providing extended soft tissue manipulation to prolong the benefits of manual therapy administered within the clinical setting.
Latex-free and wearable for days at a time, Kinesio Tape is safe for populations ranging from pediatric to geriatric, and successfully treats a variety of orthopedic, neuromuscular, neurological and other medical conditions.
The Kinesio Taping Method is a therapeutic taping technique not only offering you the support you are looking for, but also assists in the rehabilitation of injury and physiological dysfunction.
kinesio taping application:

1.Frontalis muscle:
preparation : Measure patients forehead. prepare two I strips.(cut 80% of the total length.)
ask the patient to expose the forehead pull down the skin of forehead in downward direction. stretch to the skin underlying frontalis muscles.
Application : The 1st strip : The anchor point is placed over the superior portion of forehead.only 10% or paper backing stretch is used to facilitate the frontalis muscle.
The 2nd strip : the anchor point is placed just lateral to the 1st strip. make sure 2nd strip smaller and apply with a slight stretch.
Important : The recailing of the tape occurs in superior direction this resulting in facilitation of frontalis muscle contraction.
2.Orbicularis oculi muscle:
Preparation : Measure patients oculi area. prepare four small I strips ( cut 80% of the total length ). ask the patient to close the eyelid with one hand and with the other hand lift the skin over the oculi area.
Application : The 1st strip : The strip is applied from medial to lateral direction with 10-15% stretch. The 2nd strip : The strip is applied from lateral to medial direction with 10-15% stretch.the lower eyelid is taped same manner with 10-15% stretch. resultant recoiling force helps in closure movement of lower eyelid.
3.Zygomaticus
Preparation: Measure from tempero mendibular joint to corner of the mouth. prepare one Y strip( cut 80% of the total length). The anchor is placed on the temparo mandibular joint.
Application : 1st strip :The patient is asked to stretch the skin in the opposite direction. the superior tail of the tape points towards the upper lip. apply with 15-20% stretch. 2nd strip : The patient is asked to stretch the skin in the opposite direction. the superior tail of the tape points towards the upper lip.apply the second lower tail in the same manner with 15-20 % stretch.
4.Orbicularis oris :
Preparation : Measure patients upper lip and lower lip area. prepare I strips. center first application.
Application : The patient is asked to open the mouth so as to stretch the muscle. the tape is applied with15-20% stretch on both the upper and lower lip. center first application no tension is applied at the ends. rub the tape after its application.
How to remove tape?
- So presently you’ve got your tape on and you’ve gotten that additional support throughout your chosen sporting activity, it’s time to need it off, so enable the United States to ease the tactic of removing physiology tape for you.
- the foremost effective tip we are going to provide once it involves removing your physiology tape is to peel the skin from the tape, not the tape from the skin.
- But in terms of the actual methodology, 1st ensure you’re removing the tape in an equivalent direction as a result of the expansion of the hair below it, and despite what you’re doing don’t rip the tape off kind of a plaster!
- Start slowly, folding the corners of the sting back bit by bit, guaranteeing that you’re birth the removed tape on the rear of the applied tape, as opposition propulsion the tape on top of and aloof from your arm.
- As you’re scraping the tape, hold your skin down beside your completely different hand and either regulator it or pull it gently among the opposite means of the tape. This helps the skin and so the tape to separate heaps expeditiously but with no discomfort.
- If the tape has been applied over a furred region of the body, it helps to maneuver on the tape as you are peeling it off, as a result of the pressure helps avoid a lot of pain.
- It’s knowing have shaved the realm before applying the tape but, as this isn’t frequently smart, taking this precaution square measure reaching to be necessary to some.
- want a bit additional assistance? Apply oil directly onto the tape, rub it in and wait around 10 to twenty minutes before removing it slowly. This will facilitate reducing the viscousness of the tape and build it easier to induce obviate.