
Coleman Block Test of Ankle Joint
Table of Contents
Introduction
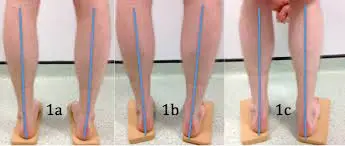
The Coleman Block Test assesses forefoot pronation and hindfoot flexibility. The forefoot has the initial malformation, whereas the hindfoot alters later.
The test involves placing the patient’s foot on a 2.5–4 cm thick wood block, allowing the first, second, and third metatarsals to hang freely into plantar flexion and pronation, and placing the patient’s full weight on the block at the heel and lateral border of the foot.
Purpose
When treating the high-arched (cavus) foot, the aim is to achieve a plantar-grade foot with the least amount of tendon imbalance by extra-articular techniques. This necessitates assessing any imbalances and coexisting deforming factors that might be causing the malformation. There are numerous conceivable combinations of contributing elements.
These include Fixed hind foot varus with secondary first ray plantar flexion necessitating hind foot correction that may result in passive correction of the forefoot; First ray plantar flexion with compensatory flexible hind foot varus, where the elevation of the first ray can lead to passive correction of the hind foot; First ray plantar flexion and fixed hind foot varus require joint forefoot and hindfoot adjustments for foot balance.
Any of these may also be linked to primary or secondary superadded tendo-achilles (TA) tightness, which may exacerbate the hindfoot’s varus deformity. This could indicate that further TA lengthening or gastrocnemius recession is needed to counteract the forces of the hind foot and put the heel into a neutral weight-bearing valgus talocalcaneal angle.
The Coleman Block Test, originally published in 19771, is used to differentiate between cavo-varus feet with a fixed hindfoot deformity and those with flexible hind feet during the physical examination. In order to administer the test, the patient’s heel and lateral border are placed on a 2 to 4-cm thick block, leaving their first, second, and third metatarsals swinging freely in plantar flexion and pronation.
The supporting block eliminates the impact of forefoot deformity (first metatarsal in fixed plantar flexion) on the hind foot stance, which is the underlying assumption that guides test interpretation. The hind foot must be flexible if the heel varus corrects while bearing weight on the block.
Correcting plantar flexion of the first ray should result in passive hind foot correction and the restoration of a neutral valgus weight-bearing tibial-calcaneal angle. The hind foot is considered inflexible if the hind foot varus does not adjust during the Coleman Block Test. This implies that in order to obtain a neutral, balanced heel posture, adjustment of the forefoot and hindfoot will be necessary.
During the normal Coleman Block Test, patients with tendo-achilles tightness in addition to plantar flexion of the first ray would produce a residual varus force on the heel, which may hinder or prevent the rear foot’s varus correction into neutral. This could cause the tester to mistakenly believe that the hind foot has a fixed abnormality.
We propose a dynamic modification of the Coleman Block Test that, by releasing the pull of the gastrocnemius muscle and so lowering tendo-achilles tension, will assist in assessing the degree of correctable hind foot varus in this case. This makes it easier to assess if first ray elevation and gastrocnemius recession will be enough to produce a balanced, neutral hind foot.
Technique:
The Dynamic Coleman Block Test
first to be able to comfortably squat, the patient must have enough pain-free range of motion in their ankles, hips, and knees. Once the patient has carefully completed the normal Coleman Block Test and made sure that equal-height blocks are under both feet to allow for neutral balance, the patient is asked to crouch down with their knees bent about 20 to 30 degrees.
By relaxing the gastrocnemius muscle’s femoral origins, this approach will lessen TA tension. A certain amount of ankle dorsiflexion and strain in the TA may result from the patient leaning too far forward or squatting too deeply. For elder patients, the test can be adjusted by pushing forward while seated in a chair.
Interpretation
Similar to the conventional Coleman Block Test, the examiner gives the results while standing behind the patient. A level of hindfoot flexibility is verified if the heel position is seen to shift into reduced varus or valgus. In this case, tightness in the TA—more especially, tightness in the gastrocnemius—must account for at least some of the deformities of the hindfoot.
Evidence
The cavo-varus foot with a flexible making-up hind foot deformity and the cavo-varus foot with an apparent fixed hind foot deformity can be distinguished using the Coleman Block Test. Forefoot procedures are typically sufficient in the former group to achieve foot balance. Two subgroups are identified by the proposed Dynamic Coleman Block Test among individuals who on the Standard Coleman Block Test appear to have an inflexible hind foot varus.
The rear foot abnormality in the first subgroup is genuinely fixed, necessitating forefoot and hindfoot treatments in order to maintain foot balance. The second subgroup maintains residual hind foot flexibility, which is disguised by TA tightness during the normal Coleman Block Test. First-ray plantar flexion and gastrocnemius recession may be adequate in this group to accomplish weight-bearing valgus tibiocalcaneal angle and balance the hindfoot.
When using this technique, it’s important to take into account the effect of ankle dorsiflexion, which should tend to increase tendon-achilles tension by tensing the soleus, which could be expected to counteract the tendo-achilles tension that is relaxed through knee flexion and gastrocnemius relaxation. It’s interesting to note that clinically, this doesn’t seem to matter, and in reality, TA tension appears to be successfully relieved by a knee bend of 20 to 30 degrees.
The presence of the largest portion of the talus within the ankle mortice is one benefit of ankle dorsiflexion. After the ankle joint is stabilized, the sub-talar joint must subsequently undergo tibio-calcaneal angle correction. This is significant because individuals who have a fixed subtalar joint may experience ankle joint laxity, which permits a degree of valgus correction because of talar tilt inside the mortice.
The talus is not stabilized within the mortice during the usual Coleman Block Test (with the ankle plantargrade), and as a result, a degree of talar tilt and valgus movement at the ankle to compensate for sub-talar joint stiffness is conceivable. Since the ankle joint is stabilized by engaging the broadest portion of the talus within the mortice in the Dynamic Coleman Block Test, any correction into valgus that is seen is most likely the result of actual sub-talar joint motion.
Conclusion
It is easy to count the Dynamic Coleman Block Test, a quick and easy procedure, into a typical foot and ankle evaluation. It gives more details regarding the nature of hind-foot deformity and is a supplement to established methods.
It helps plan surgical treatment and can show whether tendon-achilles tendon tightness is masking hind foot flexibility. In particular, it can assist in determining whether the combination of first ray elevation and gastrocnemius recession will result in a balanced, neutral hind foot.
FAQ
What is the Coleman block test?
Patients with a Cavo varus foot deformity can perform the Coleman Block Test, which was originally described in 1977 by Sherman Coleman, MD, and William Chestnut, MD, to assess if the hindfoot varus deformity is flexible or fixed. It aids in determining the kind of orthotics needed and whether surgical intervention is necessary.
What is the special test for pes cavus?
Clinical Exams
The subtalar joint’s flexibility is assessed using the Coleman block test. During the test, the patient is made to stand with a 1-inch wood block beneath their lateral and heel feet. This permits plantar flexion of the initial ray off the block.
How is Cavovarus’s foot diagnosed?
Clinical diagnosis occurs when a foot deformity with cavus, hindfoot varus, plantarflexion of the first ray, and forefoot adduction is present. To help with surgical planning, the flexibility of the hindfoot deformity can be evaluated using the Coleman Block Test.
What is the significance of the Coleman Block test?
To determine whether an inverted heel is caused by a forefoot problem, such as a plantarflexed first ray, one can do the Coleman block test, which involves supporting the lateral forefoot. The lateral forefoot may need to be brought to the ground by inversion of the heel due to a rigid plantarflexed first ray.
Reference
- Lawton, R. (2014, June 1). The dynamic coleman block test: a novel examination technique for cavo-varus feet. http://www.research-journal.net/en/The-dynamic-coleman-block-test-a-novel-examination-technique-for-cavo-varus-feet.html
- Coleman Block Test. (n.d.). Physiopedia. https://www.physio-pedia.com/Coleman_Block_Test
- Coleman Block Test. (2020, July 22). Wheeless’ Textbook of Orthopaedics. https://www.wheelessonline.com/bones/foot/coleman-block-test/
- Foran, I. M., Mehraban, N., Jacobsen, S. K., Bohl, D. D., Lin, J., Hamid, K. S., & Lee, S. (2020). The effect of the Coleman Block Test on Adult Hindfoot Alignment was evaluated using weight-bearing computed tomography, radiography, and clinical examination. Foot & Ankle Orthopaedics, 5(3). https://doi.org/10.1177/2473011420933264
- O. (2022, May 8). Coleman Block Test | OrthoFixar 2023. OrthoFixar. https://orthofixar.com/special-test/coleman-block-test/





