Wrist Instability
Table of Contents
What is a Wrist Instability?
Wrist instability is a complex and often debilitating condition that affects the wrist joint, compromising its ability to provide support and mobility for the hand and forearm. This condition arises when the ligaments, tendons, or bones that make up the wrist joint are compromised or damaged, leading to a loss of stability and control.
The wrist is a crucial anatomical structure, facilitating a wide range of hand and forearm movements essential for daily activities, including gripping, lifting, and rotating objects. It is composed of eight small bones called carpal bones, which are connected by ligaments and tendons. These structures work in harmony to provide stability and flexibility to the wrist joint.
Wrist instability can result from various causes, including traumatic injuries, chronic overuse, congenital conditions, or degenerative changes over time. Understanding the underlying cause of wrist instability is crucial for determining the most appropriate treatment approach.
This condition can manifest with a variety of symptoms, including pain, weakness, limited range of motion, and an overall reduction in wrist function. Left untreated, wrist instability can significantly impact an individual’s quality of life and hinder their ability to perform routine tasks and engage in recreational activities.
In this series of articles, we will delve deeper into the causes, symptoms, diagnosis, and treatment options for wrist instability. We will explore surgical and non-surgical interventions, rehabilitation techniques, and lifestyle adjustments that can help individuals regain wrist stability and functionality.
Introduction
- The wrist complex is a highly complicated structure. It has many small carpal bones and joint structures. It has 3 degrees of motion (flexion-extension, radial deviation-ulnar deviation, rotation). The wrist remains remarkably stable even with multidirectional external forces.
- The wrist maintains the balance between physiological forces and articulations due to intrinsic ligaments and extrinsic ligaments. The considerably high loads lead to an imbalance of equilibrium, and instabilities of carpal bone develop.
- There are two types of instability present.
- The first one is dynamic instability which happens only when the wrist is in motion
- the second one is static instability which is defined as the instability that occurs when the wrist is at rest. the main types of instability are radio-carpal and mid-carpal instability.
Understanding Wrist Anatomy
There are eight carpal bones in your wrist. there are divided into two rows; proximal and distal. the proximal row of the carpal bone is scaphoid, lunate, triquetrum, and pisiform (moving from radial to ulna), while the distal row of the carpal bone is (trapezium, trapezoid, capitate, and hamate).accompanied by the scapholunate ligament and the triangular fibrocartilage complex. These components are essential for maintaining wrist stability, enabling you to lift and use your hand for a multitude of task
Causes of Wrist Instability
Acute Ligamentous Instability
- Trauma
- Indirect loading injury
Acute Bony Instability
- Fractures
Chronic Instability
- Repetitive microtrauma
- Post-traumatic sequela (distal radius fracture)
Systemic Illness
- Avascular necrosis of the scaphoid
- Rheumatoid arthritis
Neurological
- Typically through the emergence of neurogenic arthropathies, or Charcot-like joints
- Syringomyelia
Congenital Instability
- The Madelung deformity causes misalignment of the forearm (radius, ulna) and carpal bones, predisposing to progressive arthrosis and instability.
Mechanism of Wrist Instability
Carpal Instability Dissociative (CID)
- Instability is defined as instability in bones in any single carpal row. It may involve either the proximal or distal carpal rows It is classified into two types.
1) Scapholunate (SL): The most common mechanisms for injury are Wrist extension, ulnar deviation, and carpal supination.
2) Luno-triquetral (LT): Lunotriquetral ligament, radio-lunate ligaments (both volar and dorsally), and dorsal intercarpal ligaments play a key role in this joint stability.
Carpal Instability Nondissociative (CIND)
In CIND, there is no specific difference between proximal and distal carpal rows. Instead, it may involve the whole of the carpal row, either from the radiocarpal joint, or the mid-carpal joint. or both. It is classified into two types.
- CIND-VISI: There are three carpal bones in the proximal row which rotate from flexion to extension position when the wrist goes into radial deviated to ulnar deviation position. the whole movement is maintained by wrist ligaments extrinsic ligaments (triquetral-hamate-capitate ligament, dorsal radio-triquetral, and the anterolateral scaphotrapezial ligament), and intrinsic ligaments (ulno-lunate and lunotriquetral).
- CIND-DISI: The damage of Dorsal intercarpal ligament, long radio-lunate, radioscaphocapitate ligament, and Scapholunate ligament (Intrinsic) results in dorsal subluxation of the capitate.
Sign and Symptoms
- Painful clunking
- Swelling and or deformity
- Pain in the push-up position
- Weakness in grip
- A sensation of the wrist giving way
- Paresthesia, along with the distribution of median nerve
Diagnosis
Examination
- Snuffbox tenderness
- would indicate a possible scaphoid fracture
- Dorsal intercalated segment instability (DISI) tests
- Pain with extreme extension and radial deviation
- Dorsal wrist pain with loading
- Tenderness distal to Lister tubercle (scapholunate disruption)
- Watson Test: The wrist should be in slight extension. then the patient’s wrist is moved from ulnar to radial deviation and at the same time the examiner will feel a ‘clunk’ and the patient experience pain if the test is positive. for the completeness test, the test must be performed on both wrists for the comparison.
Volar intercalated segment instability (VISI) tests
- LT Shuck test (ballottement test):
- Once the lunate is balanced, the wrist is taken by active and passive radial and ulnar deviation. The test is successful if there is pain or clicking at the lunotriquetral joint.
- Lunotriquetral compression test:
- During radioulnar deviation, the triquetrum is displaced ulnar, causing discomfort.
Carpal instability nondissociative (CIND) tests
- The sudden shift of proximal row into extension with ulnar deviation of the wrist.
Distal radioulnar joint instability
- Painful compression of ulna against radius
Piano Key Test:
- In the piano-key examination, the wrist is placed into pronation and the hand is stabilized. check the dorsal ulnar prominence relative to the radius must be done and then the ulnar head must be pushed in a volar direction. the test must be performed on both wrists for comparison. The test is noted positive when a minimal amount of resistance is felt against the volar displacement of the ulnar head and characterized by painful laxity of the affected wrist (DRUJ)
- Generalized ligamentous laxity may be present.
- If the median nerve is compressed, the Tinel sign may be positive.
Evaluation
Blood
Routine labs as a baseline
Rheumatoid factor and
Other connective tissue markers
CRP and WC for any kind of chronic inflammation or infection
Imaging
The following radiograph views are recommended
- Anterior-posterior (AP)
- Lateral
- Clenched fist
- Scaphoid
- Radial and Ulnar deviation
- Flexion and Extension
CT Scan
MRI (Magnetic resonance imaging)
Differential Diagnosis
A painful wrist with clunking and weakness and with or without trauma would have a wide range of differentials. These include the following:
- Painful ganglion
- Carpal fractures
- Stress fractures
- Ulnar impaction syndrome
- Essex-Lopresti Injuries
- Galeazzi fractures
- Kienbock disease (lunate avascular necrosis)
- Tendinitis
- Distal ulnar fracture
- Ulnar collateral ligament sprain
- Tringular fibrocartilage complex lesion
- Lunotriquetral instability
- Distal radioulnar joint injury
- Pisotriquetral joint injury
- Extensor carpi ulnaris thendinopathy or subluxation
Complications
Perilunate Dislocation
- Median nerve compression
- Compartment syndrome
- Lunate ischemia
- Avascular necrosis of the lunate
Radiocarpal Instability
- Acute carpal tunnel syndrome
- Wrist stiffness
- Wrist joint arthritis
- Chronic instability
- Wrist deformities
DISI (Dorsal intercalated segment instability)
- Scaphoid nonunion advanced collapse
- Scapholunate advanced collapse
- Wrist joint stiffness
- Wrist joint arthritis
- Weak Wrist grip
VISI (Volar intercalated segment instability)
- Wrist stiffness
- Loss of dart-throwing mechanism
- Chronic Instability
DRUJ (Distal radioulnar joint instability)
- Distal radioulnar arthrosis
- Chronic pain at the wrist joint
- Painful supination/pronation
Treatment of Wrist Instability
Conservative treatment
- immobilization
- Closed Reduction and Splinting
- NSAIDs
- Anti-inflammatory drugs
Physiotherapy Treatment for Wrist Instability
During immobilization
- Adjuncts such as moist heat, warm socks, cryotherapy with ice massage, and transcutaneous electrical nerve stimulation (TENS) could also be applied for pain relief and decreased edema.
- This will also help prevent joint stiffness
- Full range passive as well as active movement of elbow and shoulder
During mobilization
- Soothing heat therapy using a hydro collator pack and paraffin wax bath induces relaxation, improves local circulation, and puts the wrist and forearm in ideal stimulation for exercise.
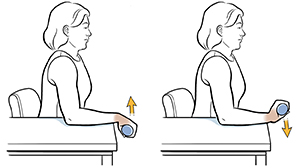
- Isometrics exercise
- Full-range movements of elbow and shoulder
- Wrist-wrist mobilization initiates with a small range of relaxed speedy flexion extensions.
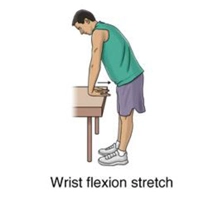
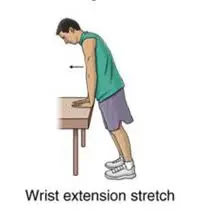
- Self-assisted stretching of wrist muscles
Surgical treatment
- Soft tissue reconstruction
- Reduction & Pinning
- This is required in unstable DRUJ injuries Arthroscopic/Open Debridement
- If TFCC injuries are not treated by conservative management arthroscopic surgery or open debridement is required for the treatment.
Radiolunate Fusion
- Radiolunate fusion, removing the painful clunking while maintaining a good range of dart-throwing motion.
Wrist Arthrodesis
- It is a procedure in which the fusion of the radius bone and the carpal bones mobilizes the wrist joint.
Physiotherapy Treatment
During immobilization (3-4 weeks)
- The period of immobilization is longer so precautions should be taken to maintain strength and regain full ROM (Range of motion) of the uninvolved joint of the affected limb.
- Immobilised by POP(plaster of pairs)
- Check the alignment of the affected limb
Mobilization (after 4 weeks)
- The movements are more painful after the immobilization. this could be helped by thermotherapy before and after the exercises. such as moist heat, warm socks, cryotherapy with ice massage, and transcutaneous electrical nerve stimulation (TENS) could also apply
- Isometrics
- Full range movements of elbow and shoulder.
- Isometrics exercise with weight for increased muscle strength.
- Wrist-wrist mobilization initiates with a small range of relaxed speedy flexion extensions.
- Self-assisted stretching with the palm at the end of the table
- Self-assisted Supination and pronation on table
Home advise
- Take frequent breaks from activities that make your pain worse.
- Apply heat to reduce pain.
- Do not lift heavy weight on the affected wrist.
Summary
- This is a condition where the wrist experiences abnormal movement, often resulting from an injury to specific ligaments that leads to the misalignment of bones. The primary ligaments that typically get involved are the scapholunate ligament(SL) and the triangular fibrocartilage complex(TFCC).
FAQs
What provides stability for the wrist joint?
The ulnar and radial collateral ligaments, along with the palmar and dorsal radiocarpal ligaments, are the four ligaments in responsible for ensuring the stability of the joint.
How long does it take for the wrist to heal?
In the conservative approach, it takes 2-3 months to heal and in the surgical approach, it should take 6 months of duration.
Why is wrist stability important?
Our wrists are responsible for positioning our hands to facilitate function and movement and tolerating heavy loads that allow us to lift, carry, push, and weight through our arms. To do their job properly, wrists need to be strong and stable.
How can we improve wrist mobility?
Rotate the wrist down and from side to side
Stretch the fingers far apart, relax them, then stretch them again.
Stretch your thumb by pulling it back gently holding it and then releasing it.What causes a weak wrist?
Carpal tunnel syndrome,
arthritis,
peripheral neuropathy, and
ganglion cysts.