
Painful arc syndrome: Physiotherapy Treatment
Table of Contents
What is Painful arc syndrome?
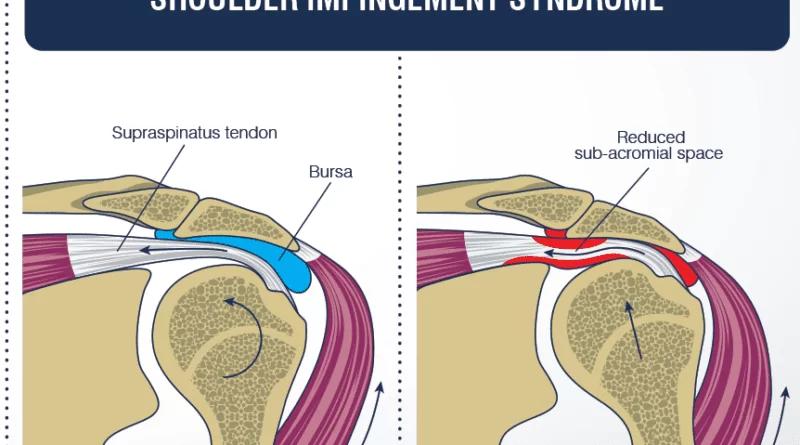
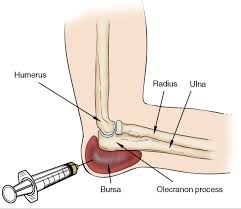
Painful arc syndrome occurs in the shoulder, The shoulder joint owes its stability to the ‘rotator cuff’ muscles – which are four small muscles located around the shoulder joint which help with movement, but importantly their tendons stabilize the head of the humerus within the joint capsule. Sometimes, with wear and tear supraspinatus tendinitis results, which is commonly associated with inflammation of the bursa also called subacromial bursitis. There may even be little tears in the tendon fibres – partial tears or sometimes even complete tears. It is typically seen in people aged 25-60.
Painful Arc syndrome, also called shoulder impingement syndrome, subacromial impingement, supraspinatus syndrome, swimmer’s shoulder, and thrower’s shoulder. It is a clinical syndrome that occurs when the tendons of the rotator cuff muscles become irritated and inflamed as they pass through the subacromial space, the passage beneath the acromion. This can result in pain, weakness and loss of movement at the shoulder.
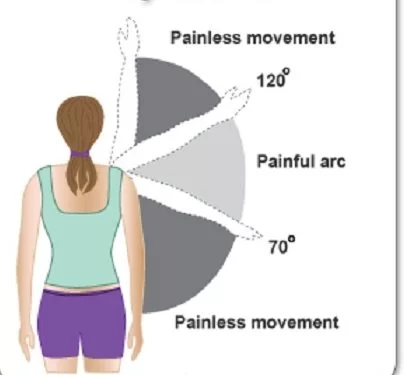
Tendinitis and partial tears in the supraspinatus tendon cause a ‘painful arc’ since as the person elevates his arm sideways, the tendon begins to impinge under the acromion throughout the middle part of the arc, and this is usually relieved as the arm reaches 180 degrees (vertical).
Painful arc syndrome causes :
- Minor tear of the supraspinatus muscle
- Supraspinatus Tendinitis
- Calcification of supraspinatus muscle
- Subacromial bursities
- Fracture of greater tuberosity
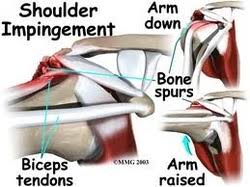
- Subacromial spur
- Tilting of the humeral head
When the arm is raised, the subacromial space (a gap between the anterior edge of the acromion and the head of the humerus) narrows, through which the supraspinatus muscle tendon passes Anything causes further narrowing the tendency to impinge the tendon and causes an inflammatory response, resulting in impingement syndrome.
Painful arc syndrome symptoms :
- The most common symptoms of impingement syndrome are Shoulder pain, weakness, and a loss of movement at the affected shoulder Joint.
- The pain is often worsened by shoulder overhead movement and may occur at night, especially if the patient is lying on the affected shoulder.
- The onset of the pain may be acute if it is due to an injury or may be insidious if it is due to a gradual process such as an osteoarthritic spur.
- The pain has been described as dull rather than sharp, and stays for long periods of time, making it hard to fall asleep at night.
- Other symptoms can include a grinding or popping sensation during movement of the shoulder.
- The range of motion at the shoulder may be limited by pain. A painful arc of movement may be present during the abduction of the arm from 60° to 120°.
- Passive movement at the shoulder will appear painful when a downwards force is applied at the acromion but the pain will ease once the downwards force is removed.
PROGRESSION :
The tendinitis results from trauma (e.g. a fall, dog on leash) in around 30% of cases.
5% of cases are bilateral.
The pain will severely limit shoulder movement and may cause secondary muscular neck pains.
DIAGNOSIS :
Plain X-rays of the shoulder can be used to detect some joint pathology and variations in the bones, including acromioclavicular arthritis, variations in the acromion, and calcification. However, x-rays do not allow visualization of soft tissue and thus hold a low diagnostic value.
Ultrasonography, arthrography, and MRI can be used to detect rotator cuff muscle pathology. MRI is the best imaging test prior to arthroscopic surgery.
The physician may inject lidocaine (usually combined with a steroid) into the bursa, and if there is an improved range of motion and a decrease in pain, this is considered a positive “Impingement Test”.
Impingement syndrome can usually be diagnosed by history and physical exam. On physical exam, the physician may twist or elevate the patient’s arm to test for reproducible pain through some special tests. These tests help localize the pathology to the rotator cuff, which is –
- Neer test
- Hawkins-Kennedy test
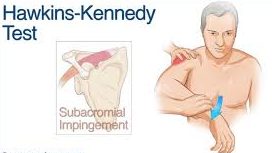
However, they are not specific for impingement. Neer signs may also be seen with subacromial bursitis.
Painful arc syndrome treatment :
Impingement syndrome is usually treated conservatively, but sometimes it is treated with arthroscopic surgery or open surgery. Conservative treatment includes –
- Rest: to allow the inflammation to settle
- Analgesics such as NSAIDs – naprosyn 250mg three times daily with food.
- Injection of corticosteroid with local anesthetic into the subacromial bursa or the supraspinatus tendon itself will help (though there may be an increase in discomfort in the first 48 hours).
- Physical therapy
Surgical Treatment
A number of surgical interventions are available, depending on the nature and location of the pathology.
Surgery may be done arthroscopically or as open surgery.
The impinging structures may be removed in surgery, and the subacromial space may be widened by resection of the distal clavicle through acromioplasty – i.e. re-shaping the acromion and excision of osteophytes on the under-surface of the acromioclavicular joint. Damaged rotator cuff muscles can be surgically repaired.
Physiotherapy treatment :
Physiotherapy treatments would typically focus on maintaining range of movement, improving posture, strengthening shoulder muscles, and reduction of pain.
Patients who present with SIS will have shoulder pain that is exacerbated with overhead activities. Pain will be the patient’s chief complaint and thus relieving pain will initially be the primary goal of physiotherapy. Patients with SIS will present with a painful arc of motion (shown to the right). This arc is from 60-120 degrees of shoulder abduction.
For Pain Relief :
Educating the patient on avoiding this painful ROM with repetitive tasks is key to the initial stages of decreasing pain in the shoulder.
- Ice pack / Hot Pack
- Joint Mobilisation – grade 1 & 2 glide
- SWD (Short Wave Diathermy)
- Ultrasound Therapy
- TENS
- IFT (Interferential Therapy)
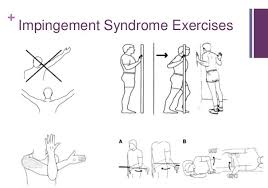
Painful arc syndrome exercises :
For ROM Improvement :
- Active assisted movement of the shoulder joint for 5-7 days
- The patient has anterior instability and tightness of the posterior capsule. So, performing stretches into IR will allow patients to regain full ROM into IR.
- Joint Mobilization with PA grade III/IV

- Functional Activities like wearing clothes on their own, doing overhead activities, and postural education may be needed.
- Therapeutic Taping
For Strengthening of muscles:
- Resisted exercise for IR, ER, ABDUCTION, SCAPULAR RETRACTION, ELEVATION
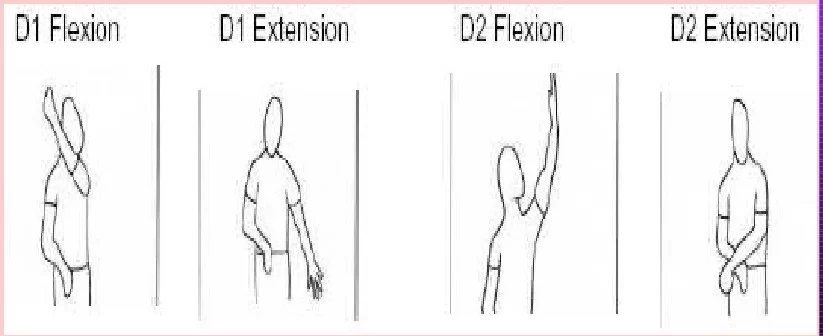
- PNF techniques for shoulder joints – may provide benefits in more functional patterns.
Special Instructions :
Most importantly with patients who are experiencing SIS, avoiding painful activities is the most important instruction. Aggravating the already inflamed, irritated shoulder joint is what must be avoided. Examples of potentially painful positions are:
Instruct the patient to avoid sleeping on the involved shoulder as this will place compressive forces through the shoulder and will exacerbate the pain.
Instruct the patient to avoid repetitive overhead activities outside their pain-free ROM. (i.e. putting groceries away overhead, reaching for items in taller closets, hammering nails into the wall above head, lifting children up above their heads).



One Comment