Concave Convex Rule
In physical therapy programs, the convex-concave rule is often discussed in the context of joint mobilizations or manipulations. The rule provides guidance on how the shapes of joint surfaces (convex or concave) affect the direction of movement during joint mobilization techniques.
- The convex-concave rules of arthrokinematics have been studied for about 30 years in physical therapy programs in the United States of America. The works of MacConaill, Maitland, Basmajian, and Steindler can be used to substantiate the claim that the morphology of articular surfaces has a close relationship to kinematics.
- These early studies of the structure and functioning of skeletal joints, or arthrology, as a field of study, together with those of others, contributed to the discipline’s definition.
Here’s a brief explanation of the rule in the context of arthrokinematics and physical therapy:
- Convex-on-Concave: When a convex joint surface moves on a concave joint surface, the convex surface moves in the opposite direction to the overall joint movement. This relationship occurs in many joints, such as the shoulder and the knee.
- Concave-on-Convex: When a concave joint surface moves on a convex joint surface, the concave surface moves in the same direction as the overall joint movement. An example of this relationship can be found in the radiocarpal joint of the wrist.
Table of Contents
Introduction
- ‘Arthrokinematics’ refers to how joint surfaces move. The two are different in arthrokinematics. In general, bone movement is referred to as osteokinematics, while joint movement is referred to as arthrokinematics.
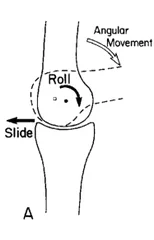
- Rolls, Spins, and Slides work together to cause the angular movement of bones in the human body.
- Roll: One bone moving over another is known as a roll.
- Spin: One body spinning on another is known as a spin.
- Slide: A slide is a translational action in which the surfaces of two joints glide over one another.
Types of Arthrokinematic Motion
- Joint Play: Active muscle contraction cannot produce passive movement, which is a movement not under conscious control.
- Component Movement: Active motion is accompanied by obligate joint motion that occurs outside the joint. i.e.- scapulohumeral rhythm
Why Arthrokinematics Matters
- The convex-concave rule when joint mobilization gliding techniques are employed to increase a particular joint motion, serves as the foundation for defining the direction of the mobilising force.
- Whether the moving surface is convex or concave impacts the sliding direction.
- Concave = Hollowed or rounded inward
- Convex = Curved or rounded outward
- If the surface of the moving joint is CONVEX, sliding will occur in the opposite direction of the bone’s angular movement.
- Sliding occurs in the SAME direction as a bone angular movement if the moving joint surface is CONCAVE.
Convex-concave rule Examples:
- Glenohumeral articulation: Convex humeral head articulates with concave glenoid fossa, and glenoid posterior glide enhances internal rotation and flexion.
Extension and external rotation are increased by the glenohumeral anterior glide.
- Humeroradial articulation: Concave radial head and convex capitulum are articulated.
Elbow extension is increased by the head of the radius’s dorsal or posterior glide.
Elbow flexion is increased by the radius head’s volar or anterior glide.
- Hip joint: The convex femoral head and concave acetabulum articulate in the hip posterior glide, which promotes flexion and internal rotation.
Extension and external rotation are increased during the hip anterior glide.
- Tibiofemoral articulation: Convex femoral condyles interact with concave tibial plateaus.
Flexibility is increased via tibiofemoral posterior glide.
The extension is increased by the tibiofemoral anterior glide.
- Talocrural joint: Concave mortise (tibia and fibula) and convex talus articulate.
Dorsiflexion is increased by talocrural dorsal or posterior glide.
Plantarflexion is increased by talo-ventral ventral or anterior glide.
- When we move a nearby joint partner, the concave-convex rule by Kaltenborn identifies the area of the joint capsule that is stressed: A convex joint surface rolls and glides in the opposite direction when it is moving. On a concave joint surface, the roll and glide both travel in the same direction.
- Freddy M. Kaltenborn presents the Concave-Convex Rule. It explains the movements that take place within joints that have concave and convex surfaces. The rule is typically used to specify which way a limited joint should be mobilized, although there are certain problems with this approach that have been noted by various authors. The rule should instead be used as a guide to help us decide which area of the joint capsule to check or place stress on during treatment.
- The rule results from the fact that the axis of movement for a concave joint partner is outside the bone, whereas it is inside for a convex joint partner. This explains why rolling and gliding always go hand in hand. Therefore, the glide component always occurs in the opposite direction of the roll if the convex surface is moving. Because the axis of rotation is located within the convex bone portion, if we were to roll the convex bone part, it would eventually roll off its fixed concave bone part without a gliding component. The larger range of motion is achievable because the joint surfaces remain in contact with one another.
- However, if we move the concave joint partner, the gliding comment always happens in the same direction around the convex bone partner’s axis of rotation. As a result, if we just roll, the movement would be much increased but would be severely restricted by gliding in the same direction.
Does a joint experience roll and glide in accordance with the rule?
- In their study of the glenohumeral joint’s joint kinematics during the late preparatory phase of throwing, Bayens et al. (2000) discovered that the joint does not function as a ball-and-socket joint. Contrary to what we might anticipate, in their investigation, the humeral head translated posteriorly during the late cocking phase. Scarvell et al. (2019) found that contrary to what we would anticipate based on the Kaltenborn rule, knee flexion was actually associated with a posterior translation of the femoral condyles. This is evidence that the Kaltenborn rule does not appear to apply to roll and glide in a joint. This is evidence that the Kaltenborn rule does not appear to apply to roll and glide in a joint. The convex-concave rule predicts anterior gliding of the radial head, while another study by Bayens et al. (2006) noted a posterior translation of the radial head in the proximal radio-ulnar joint during supination. What explanations exist for those results?
- In the late throwing phase, the humeral head is rolling posteriorly, which will naturally move the humeral head posteriorly, according to Schumacher (2009). In this study, the humeral head’s net translation is only a few millimeters. Consider an adult-sized humeral head with a 16 cm circumference to put this into perspective. The humeral head would theoretically simply roll off the glenoid by about 4 cm if a motion of 90° of GH joint abduction occurred solely owing to a rolling motion (without contemporaneous anterior glide at the articular surface). It is obvious that there must be a considerable, synchronous anterior glide of the humeral head, and the fact that the head only travels a few millimeters is evidence of a significant glide. Therefore, the Kaltenborn rule is not contradicted notwithstanding the findings of Bayens. We must distinguish between the movement of the joint surfaces and the movement of the center of the humerus’ head in order to properly discuss rolling and gliding, for instance using dynamic radiography.
Does the rule specify the way in which we must move?
- Let’s examine a study by Johnson et al. (2007), who found that individuals with frozen shoulders had their external range of motion increased by applying the concave-convex rule:
According to the concave-convex rule of Kaltenborn, the convex part of the glenohumeral joint—the head of the humerus—will glide anteriorly during external rotation, while the concave part—in this case, the glenoid—will roll posteriorly. This is similar to the justification we have for the apprehension test. - Johnson and colleagues concluded that in order to increase external rotation, they would have to conduct posterior to anterior glides in accordance with the Kaltenborn rule. As a result, one group did joint glides from anterior to posterior, or PA glides, whereas the control group conducted AP glides. The results were unexpected because the AP control group increased external rotation ROM by 31.3° whereas the PA intervention group only improved it by 3 degrees.
- The posteriorly directed joint mobilization technique was superior to an anteriorly directed mobilization strategy for enhancing the external rotation range of motion in participants with adhesive capsulitis, despite the PA group mobilizing in accordance with the Kaltenborn rule. Pain levels significantly dropped in both groups.
- Our interpretation of this study is that external rotation may actually be more of a spin action in the joint than a roll and glide movement. In horizontal abduction, we would prefer to anticipate a pure roll and glide. The convex-concave rule was never meant to determine the direction of a manual glide that would be performed at a joint in order to best improve a specific movement, according to Neuman (2012). The rule simply specifies the arthrokinematic pattern that reduces the convex member’s natural migration of its center in the roll direction.
THE CONVEX-CONCAVE RULE MERELY DESCRIBES HOW THE 2 JOINT PARTNERS MOVE AND WAS NEVER MEANT TO ESTABLISH THE DIRECTION OF A MANUAL GLIDE
Physiotherapists should treat pathological clinical findings that are related to the patient’s complaints rather than mobilizing a problematic joint as a general rule. According to Neuman, it’s possible that the patients’ pathology-related capsular tightness led the humeral head to migrate to a more anterior resting position as usual in relation to the glenoid. The humeral head was able to be more centrally located in relation to the glenoid because the posterior glide may have preferentially stretched certain areas of the capsule. The anterior capsule may have been partially cleared as a result of this new position, enabling further external rotation. This scenario is pure conjecture, and others may be feasible, without specific information on which area of the capsule was most constricted and the location of the humeral head both at the beginning and the conclusion of the motion range.
Is the Kaltenborn principle just misapplied?
Now let’s summarise: Is the concave-convex rule of Kaltenborn incorrect or just misapplied? No, it still speaks about the role and glide of a joint when describing arthrokinematic movement. Can it be used to decide which way we should mobilize to enhance a certain osteokinematic movement? Probably not as much. The rule might be a place to start, but because of its low dependability, we will need to evaluate range-of-motion restrictions, roll, and glide separately for each patient.
Given the evidence for how manual therapy works, it might not matter which part of a joint capsule is stressed because stretching a capsule is probably not possible, and the effects on pain and increased range of motion are more likely to be accomplished through this neurophysiological mechanism.
FAQs
The convex-concave laws of joint motion are one of the foundations of physical therapy and kinesiology foundations. A convex surface moving on a concave surface rolls in one direction and glides in the opposite direction, according to this.
Tips To Remember the Difference
The most important thing to keep in mind is that concave refers to an inside curve and convex refers to an outward curve. The ‘cave’ portion of the concave is where you should put your attention. Concave refers to something that is bent inward, so just think of how the mouth of a cave curves inward.
Concave” vs. “Convex” – What’s The Difference?
Concave refers to a curving inward shape, such as the inside of a bowl. Convex refers to a curving outward form, such as the outside of a contact lens. In other words, a concave shape can be filled, whereas a convex shape produces a dome.
According to the convex-concave rule, the preferred direction of a manual glide to improve external rotation is anterior. This logic is appropriate with a simultaneous anterior slide and posterior roll during humeral head external rotation.
Saddle joints acquire their name from the shape of each bone’s ends, which have similarities to a saddle with concave and convex sections that fit together. Saddle joints have a broader range of motion than condyloid joints and may perform angular rotations.
The increasing first derivative of a convex function causes it to curve upwards. whereas a concave function has a decreasing first derivative, leading it to bend downwards.
Concave implies “hollowed out or rounded inward” and is easily recalled due to the fact that these surfaces “cave” in. The inverse is convex, which means “curved or rounded outward.” Both words have been present for millennia, although they are frequently confused.