

Test of the Joint Instability of the Wrist Joint
To assess the joint instability of the wrist joint, there are several tests that can be performed. These tests help evaluate the ligaments and structures responsible for providing stability to the wrist. It’s important to note that these tests should be conducted by a qualified healthcare professional, such as a physician or a physical therapist. Here are a few common tests for wrist joint instability:
- These tests are used to study the joint instability of the wrist joint.
- These tests are used by the physical therapist when the patient is complaining about the wrist joint.
Table of Contents
List of the test for the wrist joint instability
- Murphy’s sign
- Piano keys test
- Pivot shift test of the mid-carpal joint
- Scaphoid stress test
- Sitting hands test
Murphy’s sign:
- Purpose=This Murphy’s sign to determine the cause for lunate dislocation is its primary function.
- Technique = Sitting is the patient’s starting position for Murphy’s sign.
- The patient was then questioned about making a fist.
- if the third metacarpal’s head is level with the hand’s second and fourth metacarpals.
- Result = This situation of the sign is positive & and indicates a lunate dislocation.
- The third metacarpal would often extend over the second and fourth metacarpals.
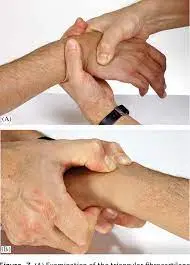
Piano keys test:

- This piano keys test is performed to determine whether the radiocarpal joint is unstable.
- Technique = The patient is seated with both arms pronated in the beginning position.
- In order to apply pressure on the distal ulna with the examiner’s index finger, the therapist stabilizes the patient’s arm with one hand.
- With the help of the other hand, the examiner (therapist) supports the patient’s hand.
- The distal ulna is pressed as if it were a piano key by the examiner.
- Results are compared to the side that is symptom-free.
- A difference in motion and the occurrence of discomfort or soreness are signs of a positive test.
- If the test is positive, the distal radiocarpal joint is unstable.
Pivot shift test of the mid-carpal joint:
- Purpose=In order to determine whether the capitate is unstable and whether the interosseous ligaments or anterior capsule have been injured, the mid-carpal joint undergoes a pivot shift test.
- Technique = The patient is seated while the pivot shift test of the mid-carpal joint is performed.
- The patient is sitting with the hand completely supinated, flexed to 90 degrees, and resting on a hard surface.
- The examiner (therapist) uses one hand to support the forearm and the other to fully radially deviate the patient’s hand while keeping the wrist in neutral.
- The patient’s hand is brought into complete ulnar deviation while the examiner (therapist) maintains the patient’s hand posture.
- Result=If the capitate moves away from the lunate, the test is positive, it suggests that the anterior capsule and interosseous ligaments have been injured.
Scaphoid stress test:

- This scaphoid stress test is a modification of the Watson test; which the patient does independently.
- The scapholunate instability & scaphoid fracture are assessed with this scaphoid stress test.
- Technique = The patient will begin the scaphoid stress test in a seated position.
- With the aid of one hand, the examiner (or therapist) supports the patient’s wrist such that the thumb exerts pressure over the scaphoid’s distal pole.
- The patient then makes an attempt to wrist radially deviate.
- Result=The scaphoid pushes posteriorly out of the scaphoid fossa of the radius as a result of excessive laxity, and the ensuing clunk and discomfort indicate a positive test for scapholunate instability or a scaphoid fracture.
- The scaphoid shift test is a passive examination carried out by the examiner.
Sitting hands test:
- The sitting hand’s press test is another name for the sitting hand’s test.
- Purpose=The sitting hands test is done to see if there is any wrist pathology or substantial wrist synovitis.
- Technique =It refers to the patient’s first sitting position.
- The patient suspends their body using only their hands for support by placing both hands on the arms of a sturdy chair and pushing off.
- The wrist joint experiences a significant amount of force throughout the test (axial ulnar load).
- This test is too demanding to pass.
- Result=The test was positive for the presence of severe wrist pathology/synovitis.
FAQ
The Piano-Key Sign Test is a test used to evaluate wrist instability clinically. It is utilized to detect wrist triangular fibrocartilage complex rips and instability of the distal radio-ulnar joint.
The tarsometatarsal joint is passively flexed and dorsiflexed while the metatarsals are held in place, as in the piano-key test. Pain or subluxation that indicates damage. Dorsal and plantar flexion of the first metatarsal head in relation to the second metatarsal head during midfoot compression.
An indication of distal radioulnar joint (DRUJ) instability known as the “piano keyboard sign” occurs when the ulnar head depresses voluntarily and then springs back into place when pressure is released. A “Z collapse pattern” is shown as the metacarpals deviate radially, the carpus translates ulnarly, and then the fingers deviate ulnarly.
Lichtman et al. provided a pivot shift test for midcarpal instability. This movement combines pronation of the wrist, axial compression, and ulnar deviation. A successful outcome of this movement is when there is a sharp wrist click.
The scaphoid shift test is a suggestive maneuver that mimics a patient’s symptoms while testing the scaphoid’s dynamic stability. Scapholunate interosseous ligament instability (SLIL) is determined with it.




