Selective Functional Movement Assessment (SFMA)
Table of Contents
Objective
- The objective of the Selective Functional Movement Assessment (SFMA) – Gray Cook and colleagues, members of the same group that developed the Functional Movement Systems, created the Selective Functional Movement Assessment (SFMA). When there is pain, the SFMA is meant to be used as a diagnostic tool for musculoskeletal evaluation. The SFMA is a clinical model that helps diagnose and treat musculoskeletal disorders by highlighting movement pattern dysfunctions.
- Physicians, physiotherapists, athletic trainers, and chiropractors are all qualified to use the SFMA. Using bodily regional interdependent movement to aggravate symptoms and reveal limitations and dysfunctions, it was developed to assess the status of movement-pattern-related pain and dysfunction.
- It identifies potential movement dysfunctions by performing a series of full-body movements. The SFMA’s objective is to evaluate the movements’ quality; The quality of the movement pattern, not the number of repetitions a person can perform, is what matters. The SFMA assists in identifying potential asymmetries and pathological patterns of movement as the underlying cause of a painful issue. A treatment strategy to restore pain-free movement and function will be influenced by this, in turn.
- Within the SFMA framework, it is essential for the clinician to comprehend the concepts of “tightness” and “weakness” in order to properly utilize the tool. “Tightness” is understood by the SFMA system to be a problem with tissue extensibility or problem with joint mobility. On the other hand, “weakness” refers to the joint’s stability and associated motor control.
- While the SFMA tool can be helpful in the initial physical evaluation of a patient, the clinician should be aware of whether the presenting signs and symptoms are acute or irritable. It’s possible that the SFMA won’t work well for an acute episode.
- The SFMA enables the evaluating clinician or therapist to pinpoint and treat areas of the body that lack stability (motor control) or mobility (range of motion), allowing for precise treatment to restore pain-free movement and function.
SFMA vs. FMS
- The Functional Movement Screen (FMS) and the Select Functional Movement Assessment (SFMA) are frequently misunderstood by clinicians.
- Although they are both components of the same Functional Movement System that Cook and colleagues developed, their primary functions are quite distinct.
- The SFMA is designed to be used as a diagnostic tool to identify pain sufferers with musculoskeletal dysfunction. In contrast, the FMS is not a diagnostic tool but rather a screening tool. During functional movements, the FMS aims to find imbalances in mobility and stability.
Scoring
- Similar to the McKenzie system, Scoring SFMA is a diagnostic system that can only be used by medical professionals.
- The Functional and Non-Painful (FN), Functional Painful (FP), Dysfunctional Non-Painful (DN), and Dysfunctional Painful (DP) ratings of the SFMA assessment are assigned to each of the seven Top Tier tests. In order to identify the true source of dysfunction, a Top Tier test that fails to pass the FN grade must move into a breakout pattern.
- To make things easier to understand, the “true cause of dysfunction” can either be a mobility problem (Tissue Extensibility Dysfunction (TED) or Joint Mobility Dysfunction (JMD) or a stability or motor control problem (SCMD).
- The SFMA may be utilized to identify remote dysfunctions through the utilization of 7 top-tier (for instance, basic movement) assessments:
- Cervical Patterns:
Flexion, extension, as well as rotation (right [R] + left [L]); - Upper-Extremity Patterns:
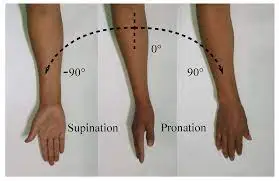
Medial (internal) rotation as well as extension pattern (R + L);
Lateral (external) rotation as well as abduction pattern (R + L); - Multi-Segmental Patterns:
Multi-segmental flexion;
Multi-segmental extension;
Multisegmental rotation (R + L); - Single-leg stance (R + L); as well as the overhead squat.
- The results of our SFMA are separated into four categories:
Functional nonpainful;
Functional painful;
Dysfunctional nonpainful;
Dysfunctional painful.
An SFMA may also be helpful to evaluate athletes in various sports like soccer, weight lifting, running, as well as baseball.
FAQs
The Selective Functional Movement Assessment (SFMA) method is a method for evaluating and categorizing movement patterns in order to properly direct manual therapy and exercise treatments. The system is made to get to the bottom of what’s causing your pain and bad movement patterns.
The SFMA is designed to be used as a diagnostic tool to identify pain sufferers with musculoskeletal dysfunction. In contrast, the FMS is not a diagnostic tool but rather a screening tool. During functional movements, the FMS aims to find imbalances in mobility and stability.
The SFMA facilitates the effective integration of posture, muscle balance, and fundamental movement system patterns into musculoskeletal practice.
The Selective Functional Movement Assessment (SFMA) is a set of seven full-body movements meant to look at fundamental movement patterns like bending and squatting in people who already know they have pain in their musculoskeletal system.
Our clinical assessment for people who are in pain is the SFMA. By logically breaking down dysfunctional movement patterns in a structured, repeatable assessment, it is a movement-based diagnostic system that finds the cause of pain rather than just the source.
The representation of core stability in the three essential foot positions that humans experience each day is shown in the first three FMS tests—the squat, the hurdle step, and the lunge. The “big three” are their names.
A functional movement screen is used by clinicians and therapists at Banner Health to find any limitations or asymmetries that could make you more likely to hurt yourself. Screening lets you know if you have a good foundation for movement and can handle more difficult exercises or activities.
Examples of fundamental movement skills are:
Balance skills are movements in which the body moves around its horizontal and vertical axes while remaining stationary.
Skills that use the hands and feet, like running, jumping, hopping, and galloping.
Ball skills such as underarm roll, striking, catching, and throwing
It is possible to classify dysfunctional movement as either a mobility deficit or a deficit in stability and motor control. Stability and motor control are the inputs required to produce an acceptable output, according to the SFMA. A lack of acceptable fundamental mobility in a joint or soft tissue structure is referred to as a mobility deficit.