Psoas Syndrome
Table of Contents
Introduction:
- Psoas syndrome is an injury to the iliopsoas muscle, typically seen in athletes, often runners, dancers, or high jumpers. It usually results from overuse and trauma. It is frequently a so known as jumpers hip and dancer’s hip. It is a frequent cause of groin pain in athletes, especially in kicking sports and adolescent athletes during an improved spurt. Furthermore, iliopsoas tendonitis following arthroscopic hip replacement iliopsoas syndrome is mainly reasonably commonplace.
- Psoas syndrome can often be secondary to iliopsoas bursitis, as well as a variety of musculoskeletal disorders and Psoas syndrome is usually a term used interchangeably with iliopsoas tendinitis, internal snapping hip, or iliopsoas impingement. Many patients respond to conservative management, but refractory cases may require advanced imaging to aid in the diagnosis, plus corticosteroid injections and surgical intervention for pain relief. Providers should keep psoas syndrome on their diagnosis for patients presenting anterior hip or groin pain with a history and physical suggestive of iliopsoas injury.
What is psoas syndrome?
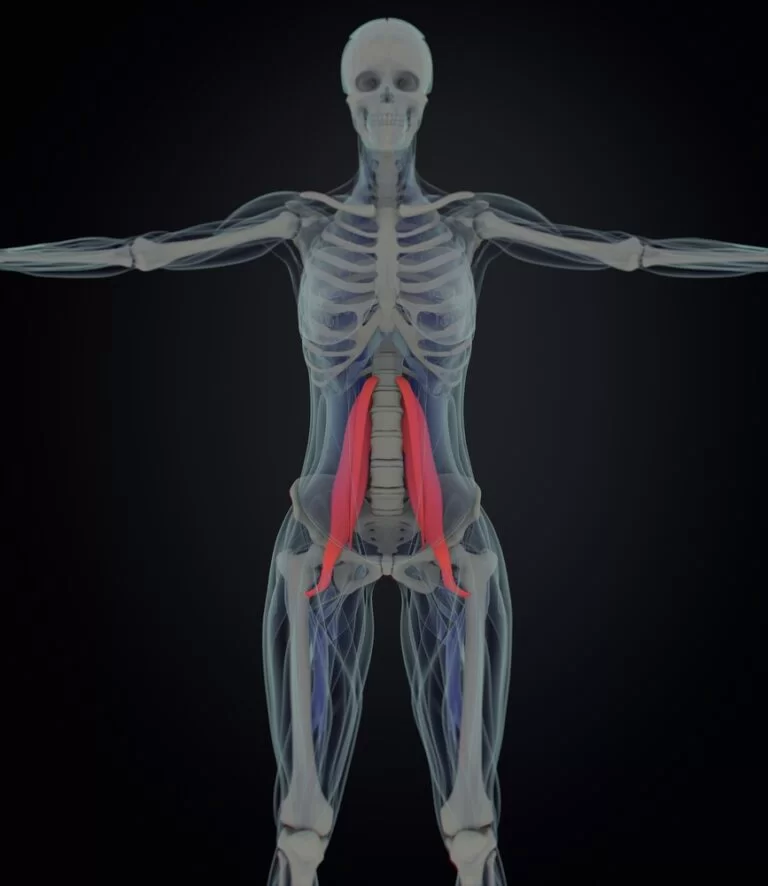
- Psoas syndrome is uncommon and often misdiagnosed, a condition that can appear as refractory lower back pain (pain that stays even after treatment) accompanied by other symptoms. This condition occurs when the psoas muscle—the long muscle (up to 16 inches) in your back—is injured. the psoas muscle is located in the lower lumbar region of the spine or extends through the pelvis to the femur. This muscle works by flexing the hip joint or lifting the upper leg towards the body.
- A most common example of the movement created by this muscle is walking. Psoas syndrome is a rare condition. Other conditions—disc herniation, arthritis, facet, and sacroiliac pain—are much more common. When those conditions are treated, often with physical therapy, the psoas muscle is stretched and strengthened. These can help treats psoas syndrome without it ever being diagnosed.
Etiology:
- Psoas syndrome is very commonly seen in athletes but can occur in the general population as well. The prevalence is higher in runners or athletes partaking in plyometric exercises. Activities that result in repetitive hip flexion can result in psoas syndrome. Psoas syndrome also occurs in patients with either inflammatory or degenerative arthritis, as well. Separately, psoas tendinitis and syndrome can occur with the impingement of the psoas tendon against an oversized acetabulum.
- The post-operatively psoas muscle tendinitis (syndrome) can occur for a variety of reasons ranging from recurrent hematomas in the iliopsoas tendon to protruding surgical screws. The location of the psoas muscle is in the lower lumbar area of the spine or has attachment points along the pelvis and femur. The primary action of the psoas muscle is it serves as a hip flexor and external rotator of the leg. This psoas muscle proximal attachment is along with the transverses processes of the lumbar spine
- . Separately, the iliac muscle proximal attachments along with the inner surface of the ilium. the muscles then insert on the medial aspect of the proximal femur and lesser trochanter. In 15% of people, the iliopsoas bursa communicates with the hip joint, and Any snapping or clunking which may occur on physical exam as the patient’s leg moves from flexion and extension is due to the iliopsoas tendon moving medially to lateral on the femoral head. This snapping of the iliopsoas muscle leads to inflammation or fluid accumulation in the iliopsoas bursa.
Epidemiology
- This incidence and prevalence of psoas syndrome in the general population are unknown. However, female athletes are at higher risk, as well as patients with hip osteoarthritis and rheumatoid arthritis. commonly speaking, hip pain is relatively common in patients 60 years of age or older, but psoas syndrome is an uncommon cause.
- The reported prevalence of the iliopsoas syndrome postoperative following a total hip arthroplasty is 4.3% in patients. this study of 252 total hip arthroplasty patients showed the incidence of iliopsoas tendonitis to be 24% of cases.
What causes psoas syndrome?
- Psoas syndrome has no identifiable cause. Care should be taken in people who are immune-compromised to ensure that there is no infectious cause and associated myositis in the psoas muscle that is present in a related fashion.
What is the symptom of psoas syndrome?
- Lower back pain, is the common symptom, although this can be symptomatic of many conditions
- Pain in the lumbosacral region when sitting and particularly when changing positions arising from sitting to standing
- The difficulty of the pain when trying to stand in a fully upright posture
- Pain in the buttocks
- Radiation of pain down the leg
- Groin pain
- Pelvic pain
- Limping and shuffling stride when you walk
- Many of these symptoms can mimic other, many serious conditions. Hip osteoarthritis, kidney stones (ureteral calculi), hernias, femoral bursitis, prostatitis, salpingitis, colon cancer, or colon diverticulitis can also cause severe back pain. It this important to consult your doctor if you have any of the symptoms.
How is psoas syndrome diagnosed?
- X-rays of the hip are often negative in the case of psoas syndrome or often unwarranted.
- Ultrasound has been helpful in the diagnostic evaluation of intraarticular versus extra-articular origins of hip pain. the lidocaine challenge test can also be useful in diagnosing psoas syndrome when the diagnosis is unclear. the ultrasound guidance, lidocaine gets injected into the psoas tendon. Reducing pain following an injection is suggestive of psoas tendonitis (syndrome).
- In 21% of athletes experiencing groin pain, iliopsoas pathology was apparent on MRI reports. If patients do not respond to conservative management of the suspected iliopsoas injury, an MRI could be beneficial in the diagnosis. MRI or US often shows an enlargement of the bursa as well as a thickening of the iliopsoas tendon.
- Labs are often in the evaluation of psoas syndrome.
Complications
- Chronic pain for untreated iliopsoas syndrome or decreased athletic performance
- Recurrent tendonitis of the iliopsoas tendon.
- Damage to the neurovascular structures of patients when a clinician performing a psoas tendon corticosteroid injection does not utilize ultrasound guidance.
Treatment
- Massage Therapy techniques involving going through the abdomen and around your iliac crests (hips) are very effective ways of treating these muscles. Your RMT will have you in the side-lying position or lying face up to best treat this muscle group. the great technique is the “pin & stretch” and “isolytic release” which involves getting you as the patient to go through either passive or active ranges of motion to optimize lengthening or repair.
- Physical exercise is also called a major component in resolving psoas syndrome. The exercises will include the active and passive spine, hip, or psoas muscle manipulation or stretching. Exercises include stretching and lower-impact dynamic exercises also known as “closed chain” which are designed to stretch and strengthen the psoas muscle or allow the body to repair & recover. When doing homecare remember to take your time or breath through movements.
Homecare
- Passive Stretch: Lie on the edge of a table or pull your knee towards you. Let the other leg hang from the edge of the table and keep it relaxed. You should feel pulling at the front of your hip and thigh. This stretch is for the hanging legs and Holds for 30 seconds. Show below for foam roller modification.

- Forward Lunge Stretch: Keep your hips square or your chest open. Do not let your knee bend past your toes and Hold for 30 seconds. See below for a deeper modification. You can add many a stretch by incorporating an anterior pelvic tilt – by tucking your buttocks underneath you and moving your pelvic bone towards you.

- Straight Leg Raise: Lying on your back, lifting one leg up while keeping your knee straight, then slowly lower your leg back down. Make sure you do not arch your lower back during the exercise. Repeat 10 if possible on both sides.

- Standing Hip Flexion: Start by standing with one leg planted and the other slightly behind you with a pulley around your ankle. Lift your legs up so that your hip or knee is bent to 90°, then slowly lower back down. Keep your hips level throughout the movements. Remembering to breathe throughout all movements.

What is the prognosis of psoas syndrome?
- With proper treatment or exercises, people suffering from psoas syndrome should be able to regain a full range of motion or resume a very high level of physical
FAQ
The symptoms of Iliopsoas tendinopathy/bursitis are: A deep aching pain felt in the front of your hip (in the crease of your hip). A clicking or clunking sensation and sound when flexing your hip (lifting your knee up). Sharp pain with sitting or standing, especially after prolonged sitting.
The psoas tendon can get inflamed from overuse, muscle tightness, or muscle weakness, resulting in a painful hip condition also known as psoas tendonitis.
Pandiculation: The many effective ways to release a tight psoas muscle. The only to change the resting level of muscle tension being set by the nervous system is through active movements. Pandiculation is mainly a neuromuscular re-education technique developed by Thomas Hanna, the founder of Clinical Somatic Education.
Direct imaging of the iliopsoas tendon is commonly performed with either MRI reports or sonography. MRI can optimally depict the psoas tendon attachment into the lesser trochanter of the femur, whereas most of the iliac attach to the proximal femoral shaft without a tendon.
There is tension in the area these nerves can be compressed as they travel through the muscles. Because tight psoas can cause seemingly unrelated symptoms including back pain, leg pain, hip pain, bladder pain, pelvic pain, or digestive issues.