
Prolapse Inter-vertebral Disc (PIVD)
Table of Contents
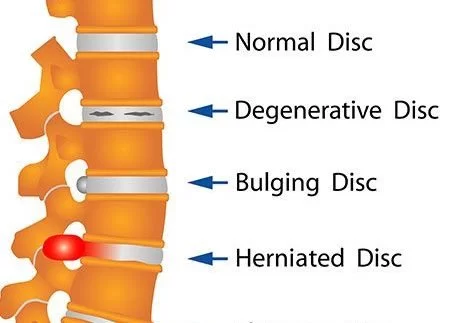
What is a Prolapse Inter-vertebral disc (PIVD)?
It is a protrusion or extrusion of the nucleus pulposus through a rent in the annulus fibrosus known as the Prolapse Intervertebral disc (PIVD).
A prolapsed disc is commonly known as a ‘slipped disc”.
The prolapsed intervertebral disc is also known as a herniated disc.
PIVD Full Name: Prolapse Inter-vertebral disc
Stages of PIVD
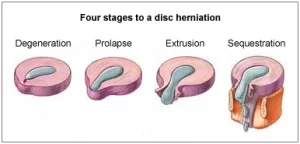
It can be divided into four stages:
The early stage is known as ‘bulging’.
The second stage can be called as ‘protrusion.
The third stage is known as ‘extrusion’.
the last stage is known as ‘sequestration’.
Pathology:
Bulging-
At this early stage, the disc is stretched and doesn’t completely return to its normal shape when pressure is relieved.
It retains a slight bulge at one side of the disc.
Some of the inner disc fibres could be torn and nucleus pulposus is spiling outwards into the disc fibres but not out of the disc.
Protrusion-
At this stage, the bulge is very prominent and the soft jelly centre has spilled out to the inner edge of the outer fibres.
Extrusion-
In the case of a herniated spinal disc, the has nucleus pulposus completely spilled out of the disc and now protruding out of the disc fibres.
Sequestration-
Here some of the nucleus pulposus is breaking off away from the disc into the surrounding area.
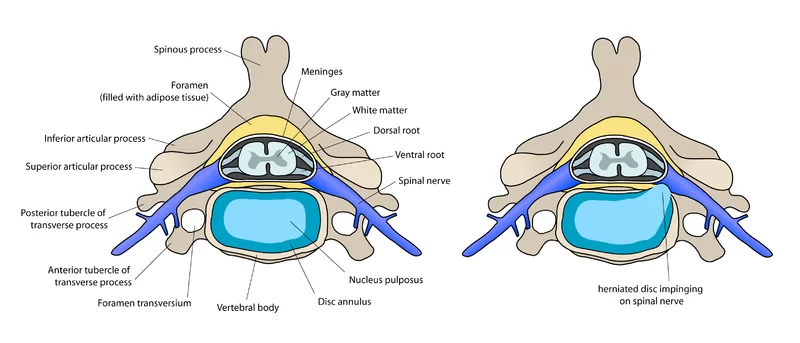
Types of herniation
(1) Central
(2) Paramedial
(3) Lateral
Causes of Disc Prolapse (PIVD):
In children may often suffer from prolapsed discs due to birth defects or injuries.
During adolescence, rapid growth leads to PIVD.
Heavy manual labour.
Sometimes playing sports like football, gymnastics, weightlifting and track and field.
Repetitive lifting and twisting.
Postural stress.
Obesity.
Poor posture and inadequate strength of the trunk.
Sitting for long hours.
increasing age
Sedentary lifestyle with alcoholic or smoking or tobacco habits
Symptoms of Disc Prolapse:
Pain in back and buttock
Weakness or numbness in one or both leg also called sciatica pain
painful or difficult walking.
From the lower back down one or both legs pain runs.
In flexion or twist pain gets worse in buttock or back.
tight hamstring muscle decreased flexibility in the lower back and pain or difficulty with arching the back backwards
Sometimes patients may often complain of sciatic pain.

Investigation:
X-ray :
decrease in the height of space between discs
nerve bundle sclerosis
bone spurs
facet hypertrophy and instability during flexion and extension of limbs.
CT Scan:
MRI Scan:
Special Tests for PIVD-
SLR test
Laesegue test
Bowstring test
Femoral stretch test
TREATMENT OF DISC PROLAPSE:
Conservative Management-
Rest: Rest and Anti-inflammatory and analgesics.
Continuing bed rest and traction for 2 weeks may reduce the herniation in over 90% of cases.
If no improvement with rest and traction, epidural injection of a corticosteroid and local anaesthetic are given.
Chemonucleolysis
PHYSIOTHERAPY TREATMENT:
Cryotherapy: reduces muscle spasm and inflammation in acute phase.
TENS: relieves pain in both acute and chronic phases.
US: as phonophoresis increases extensibility of connective tissues
Moist heat: used as an adjunct before applying specialised techniques to decrease muscle spasm.
SWD– pulsed SWD in acute condition and continuous SWD in chronic cases.
IFT-Soft tissue manipulation- to reduce local muscle spasm and induce relaxation.
Traction– may be beneficial to relieve nerve root compression and radiculopathy or paraesthesias in the acute phase of PIVD. Reduces nuclear protrusion by decreasing the pressure on the disc or by placing tension on the posterior longitudinal ligament. Time of traction should be short in acute phase else there could be an increase in disc pressure leading to increased pain due to fluid imbibition ( less than 15 minutes of intermittent traction and less than 10 minutes of sustained traction).
Local support in the form of corset: lumbosacral belt.

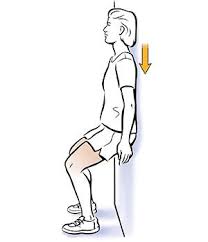
Low Back Extension Exercise :
Passive Extension
Active range of motion exercises within a pain-free range
lower limb ex. like ankle-toe movements, heel drag, hip abduction/adduction.
Isometrics of extensors
Core stability exercise:
Bridging
Leg lifts
Leg and arm raise
Wall Squat

Abdominal strengthening exercises: Isometric abs, knee to chest, bicycle exercises.
Care in Disc Prolapse : ( Do’s And Don’t):

- Back Care is Important Mainly in the Acute Phase Of PIVD.
- Rest is very important.
- Avoid Long Sitting Position. If Requires Sitting Position Use Fully Supported Chair For Sitting Position.
- Two-wheeler Driving Must Be Avoided.
- Long Driving Of Four Wheeler Must Be Avoided and in short driving use a small pillow for the low back area.
- Avoid Forward Back Bending Activity in day-to-day activity and try to use the knee instead.
- Avoid Lifting Heavyweights from the Ground and if lifting small weights keep it too close to the Body.
- Avoid painful activity, Keep Monitoring Your day-to-day activity And in which, Note which activity increases pain and try to avoid this activity.
- Avoid painful exercise.
FAQs
Treatment of Prolapsed Intervertebral Disk
Rest and avoiding activities that aggravate the pain make up conservative treatment. The majority of individuals experience significant reductions from taking Physiotherapy treatment along with muscle relaxants and nonsteroidal anti-inflammatory drugs.
Physiotherapy treatment can be effective to relieve the symptoms of PIVD (Prolapsed Intervertebral Disc) and improve a patient’s condition. Treatment outcomes may vary depending on the severity of the condition and individual factors. It’s essential to consult with a healthcare professional for a comprehensive assessment and treatment plan.
‘Slipped’ (prolapsed) discs frequently result in abrupt, severe lower back pain. The disc frequently compresses a nerve root, which can result in leg pain and other symptoms. The majority of the time, the symptoms subside over many weeks. The general advice is to keep things as normal as you can.
Four stages of PIVD –
1) Bulging disc.
2) Protrusion.
3) extrusion.
4) sequestrization
PIVD is a distinct clinical condition in which the disc material herniates into the spinal canal and the posterior longitudinal ligament breaks. The posterior longitudinal ligament may become ineffective due to vertical spinal instability or from an acute stretch carried by rapid bending or exercise.
Surgery is only ever required for a very small percentage of disc bulging patients. Through a conservative treatment plan selected by your healthcare provider on an individual basis, physiotherapy and chiropractic care can help you fully recover.
Herniated Disc Treatments Without Surgery
Injections of cortisone are given near the spinal nerves as further non-surgical therapy for a herniated disc. spasm relief with muscle relaxants. Exercises and stretches used as part of physical therapy to lessen pain.
The majority of patients with a slipped disc in their lower back are given “conservative” treatment, which means that the treatment does not require surgery. Physical Therapy Treatment, Exercise, positioning and relaxation techniques, painkillers or local anesthetics, and manual therapy are the key components of this.




