
Hiatal Hernia
Table of Contents
Introduction
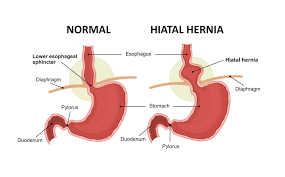
A hiatal hernia is a medical condition characterized by the protrusion of a part of the stomach through the diaphragm into the chest cavity. The muscle known as the diaphragm, which separates the chest cavity from the abdominal cavity, is essential for breathing. In a hiatal hernia, a weakened or enlarged opening in the diaphragm, known as the hiatus, allows the upper part of the stomach to move upward into the chest.
Hiatal hernias are relatively common and can affect people of all ages, but they are more commonly observed in individuals over the age of 50. There are two main types of hiatal hernias: sliding hiatal hernia and paraesophageal (rolling) hiatal hernia.
Typically, your oesophagus passes through the gap and connects to your stomach. However, if you have a hiatal hernia, your upper stomach slides through that gap and into your chest. Your stomach’s upper portion feels compressed. Through the hole, stomach acid can back up (reflux). Heartburn and other symptoms could result from this.
When bodily tissue or an organ pushes through the diaphragm, a hiatal hernia forms. The diaphragm is a membrane that separates the heart and lungs in the chest cavity from the abdominal organs and holds them in place. Between the two chambers, there is a muscle layer that has a dome-like form and moves up and down to promote breathing. Although the diaphragm has a flat surface without any open holes, it is permeated with important structures and vessels.
The food pipe, often known as the oesophagus, is the biggest of these systems. The food pipe, which links the stomach to the back of the mouth, is crucial for moving food down for digestion. The diaphragm often forms a tight seal around the food pipe just above the stomach to maintain the position of the abdominal organs and tissues. The food pipe is widened to help stop the stomach contents from rising back up into the chest portion of the food pipe. When a portion of the upper stomach pushes through the diaphragm at this location, a hiatal hernia results.
What ia a Hiatal Hernia?
When the top of your stomach pushes up through your diaphragm and into your chest, this condition is known as a hiatal hernia. The muscular wall separating your chest cavity from your abdomen is called your diaphragm. Any organ or tissue that pushes through a weakness in the tissue barrier that usually surrounds it develops a hernia. Hiatal hernias are among the most prevalent forms of hernias.
A hiatal hernia occurs when a hole develops in the muscle that divides your chest from your abdomen, the diaphragm. Considering the name of the opening, this condition is sometimes referred to as a hiatus hernia.
Your diaphragm, which is the aperture through which your oesophagus connects to your stomach, has a weakness that hiatal hernias push through. The phrase “hiatal hernia” or “hiatus hernia” refers to this hole in the oesophagus, which is what medical professionals refer to as. Over time, tension and stress may enlarge this gap. Typically, this illness takes years to steadily deteriorate.
A hiatal hernia happens when the big muscle between your belly and chest (the diaphragm) allows the top half of your stomach to protrude through. Your oesophagus (food tube) travels through the gap in your diaphragm before joining your stomach. The stomach pushes through the gap and into your chest when you have a hiatal hernia.
Generally speaking, a little hiatal hernia is not bothersome. You might not even be aware that you have a problem if your doctor doesn’t discover it when testing for another one. A significant hiatal hernia, on the other hand, can lead to acid and food refluxing into the oesophagus, which can result in heartburn.. Usually, self-care methods or medications are used to treat these symptoms. An extremely large hiatal hernia may require surgery.
Types of Hiatal Hernia
Hiatal hernias come in two main varieties: sliding hernias and fixed hernias, also known as paraesophageal hernias.
Sliding Hernia:
The sort of hiatal hernia that slides in and out is the more typical one. It happens when your oesophagus and stomach move back and forth through the gap in your chest. Small sliding hernias are typical. They typically don’t have any symptoms and might not even need to be treated.
The food pipe in your oesophagus often passes through the hiatus and connects to your stomach. Your stomach and the bottom portion of your oesophagus slip up into your chest through the diaphragm in a sliding hiatal hernia. This kind of hiatal hernia is the most common.
Fixed Hiatal hernias:
These hernias are less frequent. It is also known as a paraesophageal hernia.. A portion of your stomach pushes through your diaphragm and remains there in a fixed hernia. Most instances are not life-threatening. However, there is a chance that the blood supply to your stomach might be cut off.
The hazard from a paraesophageal hernia is greater. Your stomach and oesophagus remain in their proper places, but a portion of your stomach passes through the gap and settles adjacent to your oesophagus. Your stomach’s blood flow might be cut off if you are constricted. Your physician may refer to this as a strangulated hernia.
Causes of Hiatal Hernia
A hiatal hernia is caused by weakened muscle tissue that enables your stomach to protrude through your diaphragm. It’s not always apparent why this happens. However, a hiatal hernia might develop as a result of:
Both congenital and acquired hiatal hernias exist. The frequency is rising among the elderly. It is thought that age-related muscular weakening and elasticity loss predispose to the development of a hiatal hernia. As a result, upon swallowing, the top portion of the stomach could not return to its normal place below the diaphragm. There are other risk factors as well, such as high intraabdominal pressure. Obesity, pregnancy, chronic constipation, and chronic obstructive pulmonary disease (COPD) are the usual causes of this. Hiatal hernias can occur for a variety of reasons, including trauma, ageing, past surgery, heredity, and age
Why do Hiatal Hernia occur?
When the tissues dividing your body’s various compartments have a weak place, a hernia may result. A hernia might pass through the hole since it is weak. The oesophagal hiatus, where your oesophagus crosses your diaphragm, is where a hiatal hernia, in particular, enters the body. The only thing needed for a hiatal hernia to occur is a little expansion of this aperture.
Sometimes the initial weakness that leads to a hernia is brought on by a specific accident, surgery, or even a congenital abnormality. However, cumulative harm from years of everyday stress and pressure is most frequently the cause. Your diaphragm might gradually deteriorate due to anything that increases the pressure inside your abdominal cavity. The following are some of the most typical factors that increase abdominal pressure and lead to hiatal hernias:
- Coughing or sneezing that is persistent.
- Constipation is the ongoing struggle to urinate.
- A body mass index (BMI) of 30 or higher indicates chronic obesity.
- Vomiting a lot.
- Hard lifting or intense activity.
- Conceiving and giving birth.
- Alterations in your diaphragm caused by ageing
- Injury to the region, for instance, following trauma or certain surgeries
- Having an exceptionally big hiatus at birth
- The pressure that is repeatedly and aggressively exerted on the adjacent muscles, such as when lifting heavy objects, coughing, vomiting, or exercising.
- Damage to the vicinity
- Straining while urinating (also known as the Valsalva technique)
While preventing a hiatal hernia may not be possible fully, you can stop a hernia from getting worse by
- Reducing extra weight
- Not bending over when using the restroom
- Enlisting assistance while moving large things
- Staying away from tight belts, and avoiding specific abdominal movements
Risk factors:
Other common risk factors include obesity and the diaphragm’s ageing process.
Women, those who are overweight, and those who are over 50 are more likely to develop hiatal hernias.
Signs and symptoms of Hiatal Hernia
You probably won’t feel the hernia itself if all you have is a sliding hiatal hernia, which is what the majority of individuals experience. In contrast to other hernias, you most likely won’t see the bulge from the outside.
Hiatus hernias, especially Type I hernias, seldom cause symptoms. Burping, heartburn, nausea, and vomiting might potentially be connected to them, as well as reflux into the oesophagus.
A paraesophageal hernia or a Type II, III, or IV hernia may result in more severe symptoms. These may consist of:
- Chest/abdominal discomfort: Chest discomfort that is not cardiac. Persistent chest discomfort mimics angina but is not angina.
- Blood in the vomit, red or black stools, anaemia, or blood tests showing blood loss can all be signs of abdominal bleeding.
- Early satiety, or feeling full after only a modest quantity of food, Voice change
- Occasionally having difficulty swallowing, particularly solid meals
- Breathing issues or shortness of breath
- After eating, acid reflux
- Gagging or the experience of food sticking
Other potential indicators of a hiatal hernia might be:
- Nausea
- Acid reflux, stomach compression, or both.
- If your hernia is crushing your lungs, you may experience breathlessness.
- You may feel pressure or pain in your lower chest or upper abdomen.
- Larger para oesophagal hernias are more prone to cause these symptoms.
- Due to acid irritation, you may experience a sore throat and hoarseness when speaking.
- Both acid reflux and hiatal hernias are not always symptoms of the same condition. However, if you’ve just started to experience these symptoms more frequently, they could be connected.
Even corrected hiatal hernias seldom result in symptoms. Any symptoms you do have are typically brought on by stomach acid, bile, or air getting into your oesophagus. Typical signs include:
- Chest discomfort or epigastric pain that becomes worse when you bend over or lie down acid reflux or GERD difficulty swallowing belching
- Gastroesophageal reflux disease (GERD)-related heartburn: A heartburn that you have, especially after eating.
- Chest discomfort
- Bloating Burping: Acid refluxing back into your throat, gas, and food.
- Difficulty swallowing: Swallowing challenges or a lump in the throat during swallowing.
- Indigestion: feeling full quickly after eating and experiencing scorching belly discomfort.
- Unpleasant aftertaste
- Nausea and vomiting are experienced
- Returning food or liquid from your stomach to your mouth
- Breathing difficulty
If you have a hiatal hernia, get medical attention soon and:
- A chronic stomach ache
- Vomiting
- Unable to pass gas or poop
- These might be symptoms indicating an obstruction or a strangulated hernia, both of which are medical emergencies.
The patient’s pain and suffering are brought on by the reflux of stomach acid, air, or bile. Although there are several reasons why acid reflux happens, a hiatal hernia makes it more likely to happen.
Bochdalek hernia in infants can be identified by signs including trouble breathing, rapid breathing, and elevated heart rate.
Diagnosis:
An upper GI series, endoscopy, high-resolution manometry, oesophagal pH monitoring, and computed tomography (CT) are frequently used to diagnose a hiatal hernia. The size, position, stricture, and stenosis of the oesophagus may be visualized during a barium swallow, much like during an upper GI series. Additionally, it may assess oesophageal motions. Endoscopy can check for erosions, ulcers, and malignancies on the inside surface of the oesophagus.
Manometry, meanwhile, can detect oesophagal achalasia and assess the integrity of oesophagal motions. Acid reflux events may be quantitatively analyzed using pH testing. Diagnoses of hiatal hernia problems including gastric volvulus, perforation, pneumoperitoneum, and pneumomediastinum can be made with a CT scan.
A test or treatment to identify the source of upper abdominal discomfort, chest pain, or heartburn frequently reveals the existence of a hiatal hernia. These examinations or processes comprise:
Drink some barium: You consume a substance that appears on X-rays so that your doctor can see your stomach and oesophagus more clearly.
X-ray of the upper digestive system. After you consume a chalky substance that covers and fills the inside lining of your digestive system, X-rays are performed. Your doctor can use the coating to show your oesophagus, stomach, and upper intestine in silhouette.
A chest X-ray. The oesophagus is located inside the chest cavity, which is imaged using radiation during a chest X-ray or radiograph.
Esophagram. A video X-ray showing your oesophagus in motion is called an esophagram. When you swallow, it records a live video of the oesophagus.
The upper endoscope: A small, flexible tube called an endoscope is inserted down your throat by your doctor to inspect the interior of your oesophagus and stomach and look for inflammation. Upper endoscopy uses a small camera on the end of a long tube to see inside your stomach and oesophagus. It displays real-time visuals on a screen. An endoscope, which is a lengthy, thin tube, is inserted down your throat by your doctor. Your stomach and oesophagus are visible through the camera at the end.
.
Manometry of the oesophagus. This examination measures how often your oesophagus’s muscles contract when you swallow. The effectiveness and strength of the oesophageal muscles are also evaluated by oesophageal manometry. To measure the pressure in your oesophagus as you swallow, a different type of tube is inserted down your throat. A catheter is inserted into your oesophagus during this procedure to evaluate the muscular pressure. The information is transformed into a topographical pressure map.
A pH test: This gauges how much acid is present in your oesophagus.
Treatment of Hiatal Hernia
The majority of persons with a hiatal hernia don’t exhibit any symptoms and won’t require medical attention. You could require medication or surgery if you develop signs and symptoms like persistent heartburn and acid reflux.
Medications
Your doctor could advise the following if you frequently get heartburn and acid reflux:
- Stomach acid-neutralizing antacids: Mylanta, Rolaids, and Tums are a few antacids that might offer immediate relief. Some antacids might have negative effects if they are used excessively, such as diarrhoea or occasionally renal issues.
- Medications that lower the formation of acid: Cimetidine (Tagamet HB), famotidine (Pepcid AC), and nizatidine (Axid AR) are examples of these drugs, also referred to as H-2-receptor blockers. By prescription, stronger versions are available.
- Drugs that treat oesophagal problems and stop the generation of acid. These drugs, sometimes referred to as proton pump inhibitors, are more effective acid blockers than H-2-receptor blockers and give the oesophagal tissue time to repair. Proton pump inhibitors available over the counter include lansoprazole (Prevacid 24HR) and omeprazole (Prilosec, Zegerid). Prescription-only variants that are stronger are also offered.
The majority of hiatal hernia patients don’t need to be treated. Symptoms are often what dictate the course of treatment. If medicine doesn’t help treat your acid reflux and heartburn, surgery may be an option.
Surgery:
A hiatal hernia may occasionally need surgery. Surgery is often reserved for patients who have not found relief from heartburn and acid reflux drugs, or who have problems including severe inflammation or esophageal constriction.
Pulling your stomach into your abdomen, constricting the opening in your diaphragm, or replacing your oesophagal sphincter may be necessary during surgery to treat a hiatal hernia. In some circumstances, a sleeve gastrectomy or another weight-loss procedure is paired with hiatal hernia surgery.
Thoracotomy, a single incision in your chest wall, or laparoscopy, a less invasive procedure, are both options for doing surgery. In laparoscopic surgery, your doctor makes numerous tiny incisions in your belly and inserts a tiny camera and specialized surgical equipment. The procedure is then carried out as your surgeon watches video pictures shown on a monitor from within your body.
Medical professionals advise hernia repair surgery when:
- Your hernia results in symptoms or problems that are unaffected by medicine.
- The adverse effects of the drugs have an impact on your health and quality of life.
- Your hernia is significant enough to put you at risk for serious problems down the road.
The hernia and reflux are treated during hiatal hernia surgery by:
- Bringing your lower oesophagus and stomach back beneath your diaphragm.
- Repairing the hernia’s entry point in your diaphragm.
- Tightening the connection between your oesophagus and stomach.
The method is known as a fundoplication. The fundus, or top portion of your stomach, is referred to by this term. Your surgeon will wrap the fundus around your lower oesophagus and secure it with surgical staples or stitches throughout the surgery. The lower oesophagal sphincter, the muscle that separates the two organs, is constricted as a result. They carry out minimally invasive laparoscopic surgery whenever it is feasible.
While lifestyle modifications or medication are frequently effective treatments for hiatal hernias, some patients may require surgery to have their hernias repaired.
Your diaphragm may need to be tightened during surgery to repair a hiatal hernia in order to draw your stomach from your chest cavity back into your abdomen.
Depending on the severity of your hiatal hernia, a surgeon may advise surgery.
Among the common surgical options are:
- Surgery to correct a hiatus. The enlarged hiatus, the gap in the diaphragm through which the oesophagus passes to reach the stomach, is tightened and reduced in size during this operation using sutures and prosthetic mesh. It is used to treat early-stage hiatal hernias and stops your stomach from sagging through the hiatus.
- Fundoplication Nissen. The top component of the stomach, known as the fundus, is wrapped around the lower segment of the oesophagus using sutures in this technique to retain the stomach in place below the diaphragmatic hiatus. Your oesophagus’s end is compressed by the sutures, which stops food and stomach acid from ascending.
- Gastroplasty by Collis-Nissen. Patients who have more complicated types of Hiatal hernia caused by oesophagal shortness may benefit from this procedure to extend the oesophagus. A surgeon will expand your oesophagus during this treatment using tissue from the top portion of your stomach.
What to expect from surgery?
Hiatal hernia repair surgery normally lasts 2 to 3 hours, and it’s performed while you’re unconscious to ensure that you won’t experience any discomfort
Different surgical procedures can be used to treat a hiatal hernia:
- Fix it openly. In an open repair procedure, your surgeon will create a sizable incision in your abdomen to execute the procedure.
- Laparoscopic surgery for repair. Your surgeon will create multiple tiny cuts in your abdomen during Laparoscopic surgery, and one of the cuts will be used to implant a thin tube containing a small camera. Through further incisions, surgical instruments will be introduced.
- When performing the procedure, your surgeon will observe the inside of your stomach on a monitor that is connected to the camera.
Recovery:
After your operation, you can anticipate spending 1–2 days in the hospital. Following a soft or liquid diet and refraining from fizzy beverages for a few weeks following some procedures may be necessary.
After the procedure, you could notice that your appetite has dropped, and some patients can have diarrhoea for the first several days.
Following hiatal hernia repair surgery, there are often no severe restrictions, so you are free to walk, climb stairs, engage in sexual activity, and exercise as long as it doesn’t ache.
Depending on the sort of surgery you had, your surgeon or doctor will provide you with more detailed instructions and directions for your recuperation.
Home Remedy:
Diet:
Acid reflux symptoms are caused by a hiatus hernia. Your symptoms could disappear if you change your diet. Instead of three substantial meals throughout the day, it could be beneficial to consume multiple smaller meals. Additionally, you ought to refrain from consuming meals or snacks just before going to bed.
Additionally, some meals may make you more likely to get heartburn. Think about avoiding:
- spicy foods
- chocolate
- foods made with tomatoes
- caffeine
- onions
- citrus fruits
- alcohol
Other strategies for symptom relief include:
- Giving up smoking
- Avoid stooping or laying down after eating;
- Your bed’s head should be raised by at least 6 inches.
Summary:
Numerous sufferers of hiatal hernias are symptom-free and may not require medical attention. But for those who have more serious hernias, medical intervention, dietary adjustments, and occasionally surgery may be required to correct the hernia and relieve bothersome symptoms like heartburn and chest discomfort.
After surgery, a hiatal hernia might come back. According to 2020 research, 18% of patients who underwent a minimally invasive fundoplication surgery experienced recurrence.
You may control the symptoms of a hiatal hernia by making lifestyle changes including decreasing weight and keeping a healthy weight, stopping smoking, eating smaller quantities of food, restricting certain fatty and acidic foods, and eating meals at least three to four hours before going to bed.
FAQs:
Fortunately, it is possible to cure both acid reflux and hiatal hernias. Your hernia’s kind and symptoms will determine the course of therapy you require. Many times, taking medication and making lifestyle adjustments are sufficient to control acid reflux. You could require surgery to fix the hernia in more serious circumstances.
Although hiatus hernia issues are rare, long-term oesophageal damage from stomach acid leaks can cause ulcers, scarring, and changes to the oesophageal cells, increasing your risk of oesophageal cancer. Learn more about the problems a hiatus hernia can cause.
Hiatal hernia sufferers typically have no issues leading regular lives. However, it is crucial to consult a doctor and receive treatment if you are showing symptoms. Some hiatal hernias might cause more severe health issues if they are not addressed.
Symptoms and causes of a hiatal hernia are abdomen or chest aches. feeling full shortly after eating. respiration difficulty. blood in the vomit or dark stools, which might be signs of gastrointestinal bleeding.
Even in cases when surgery to repair a hiatal hernia is required, the process is frequently quick and effective. Most people might recover fully in a few weeks.


3 Comments