Cyclist palsy | Handlebar’s palsy:
Table of Contents
Description of Cyclist Palsy:
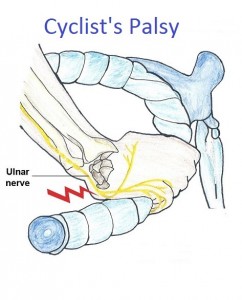
Cyclist Palsy is an ulnar nerve injury at the wrist that can occur in cyclists, in both road and mountain biking. Palsy means a nerve is being compressed and develops like some hand paralysis.
On the little finger side of the wrist, the ulnar nerve runs through a tunnel or canal, it’s called a Guyon’s Canal. In the Guyon’s canal, the ulnar nerve divides into two branches that give sensation to the little finger and the muscular branch gives the fine movements of the many more muscles in the hand. This condition occurs due to the compression of the ulnar nerve at the wrist while grasping the handlebars of a bicycle for a long period.
Handlebar palsy is known as Guyon’s Canal and it is a common condition in over-use of cycling injury. In this case, the ulnar nerve and sometimes the median nerve are also affected. In the handlebar palsy, the point injury that contact with the handlebar is involving the irritation, compression, and partial blockage of the ulnar nerve at the Guyon’s canal (little finger side of the wrist). The median nerve passes through the tunnel at the wrist, known as the carpal tunnel. This nerve also supplies the sensory and motor function to the different parts of the hands.
Cycling is a fun and healthy exercise for the fitness of our body. Whenever it can take its toll on the body with over-training and poor cycling posture or an incorrect bike fit. Hand pain is present in this condition. One research study says that 31% of cyclists experienced some hand pain due to overuse activity or long periods of cycling.
It is also known as a different name related to the condition and the symptoms are the following:
1) Handlebar palsy
2) Ulnar tunnel syndrome
3) Ulnar nerve compression
4) Guyon Canal Syndrome (GCS)
5) Bicycler’s neuropathy
6) Tardy ulnar palsy
In the cyclist’s palsy Pain, tingling, and numbness can occur in different areas such as the wrist, the little finger of the ulnar side of the hand, and the thumb side of the hand.
These symptoms are arisen due to the different causes following:
- Excessive pressure through the hands-on nerves and compression of the blood vessels.
- The wrist is held in an extended position for over some time so that stretch the soft tissue structures of the wrist.
- Insufficient core muscle strength causes excess weight on the hands and or rocking of the pelvis.
- High sitting or low handlebars cause more weight on the upper limbs.
- More vibration in the hands due to the over-inflated tires, small wheels, and skinny tires.
Causes of cyclist palsy:
Cyclists’ Palsy is generally seen in people who join in frequent cycling. Road cycling and mountain biking both are responsible for the development of Cyclists’ Palsy. When a hand is kept on the handlebars of a bicycle, the wrist is extended, because of that, the pressure arises on the nerve in Guyon’s canal at the wrist. The Cyclists’ Palsy is developed after frequent cycling over many weeks, or even after a single session during a long period.
Cyclist palsy can be the result of more vibration from the ground through your bike, causing repeated blows to the base of the palm and the amount of body weight transferred through your hands onto the handlebars. This can be worsened when the wrist is held for prolonged periods in an extended position, these places stretch on the nerve while the nerve is being compressed. It’s most commonly seen in long-distance cyclists.
Symptoms of cyclist palsy:
The irritation of the ulnar nerve can give sensory changes in your little finger side of the hand, due to that numbness and tingling are present. Riders or cyclists may have pain, weakness, cramping, and clumsiness in their hands. sometimes, In advance cases also see a clawing deformity of the hand.
Also noticeable difficulty in the use of the hand for fine motor control actions or forceful pinching. Difficulty in another activity like typing activity or playing the piano.
Compression of the motor branches of the nerves results in motor deficits, like weakness, clumsiness, and some movement limitation of the hand.
Correct and early treatment of nerve injuries are important to early recovery and the healing process can take from weeks to months depending on the severity. In case a patient does not take treatment, the nerve impingement can cause atrophy of the involved hand muscles or paresthesia of the hand muscles supplied by the nerve, it will be permanent.
Clinically Relevant Anatomy of Ulnar and Median nerve:
Ulnar Nerve:
The ulnar nerve origins from C8 and T1 of the spinal cord. The ulnar nerve is one branch of the medial cord of the brachial plexus, and it travels to the medial side of the arm, then enters the forearm. The nerve gives two branches of the hand, 1)sensory branch and 2)motor branch
The sensory branches give the sensation to the dorsomedial hand, 4th and 5th digits of fingers. The motor branch gives the fine movement of the fingers and hands.
At the wrist, the ulnar nerve enters by passing through the canal which is known as a Guyon’s Canal. This tight tunnel is formed by the ligament of the hamate, the pisiform, and the piso-hamate which helps to keep these carpal bones get together. In the cyclist, the ulnar nerve is compressed in the Guyon’s canal or just above it. The compressive injury of the ulnar nerve most commonly occurs in cyclist or riders.
Median Nerve:
The median nerve is originating from the C6 to T1 and sometimes C5 of the spinal roots. The median nerve is a branch of the medial and lateral cord of the brachial plexus. It starts from the axilla then travels into the arm and runs down and enters into the forearm. The nerve gives the different branches in the whole path.
Then The median nerve enters the hand through the carpal tunnel. Deep to the flexor retinaculum and gives the branches to the muscles of flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus. There, it is divided into the recurrent muscular branch and digital cutaneous branch and it supplies the thumb, index, middle, and ring finger of the hand. Also, give the flexion movement of the hand and pronation movement of the forearm.
The median nerve is compressed in the carpal tunnel due to any injury or overuse activity.
What are the Causes of Cyclist’s Palsy?
Cyclist’s palsy mostly develops during long-distance or prolonged periods of cycling and occurs in both mountain bike and road cyclists. Due to the hand position of the cyclist, personal pressure is generated on the nerves in the wrist while holding the handlebars for long period. While holding the handlebar the pressure generated by vibrations from the road or trails can be enough to damage or injure the compressed nerve. In most of when the cycle runs downhill, the body weight is supported by the hands on the corner of the handlebar. This position gives to a higher load on Guyon’s canal at the wrist or in the carpal tunnel.
Cyclists place their hands in a hyperextended position on the handlebar so that stretch structures of the wrist. All this can develop neuropraxia(it is a disorder of the peripheral nervous system, in which there is a temporary loss of both functions due to blockage of nerve conductivity.) One general reported that long-distance cycling may enhance the physiologic changes in the deep branch of the ulnar nerve and also gives the symptoms of carpal tunnel syndrome too.
Specific hand injury in cyclist person:
Ulnar nerve palsy:
The ulnar nerve becomes irritated and compressed in the wrist within or into Guyon’s canal, due to the pressure generated on the hands on the handlebars. Furthermore, during cycling, people keep a hyperextended position of the wrist resting on the handlebars, giving to the neuropathy by compressing and stretching the nerve as it passes from the wrist to the hand area.
The symptoms include:
- Numbness
- Tingling
- Weakness
- Clumsiness
- Cramping
- Pain
- Movement limitation
The term palsy is used because cyclists have develops hand muscle paralysis. This condition affected both sensory and motor functions of the hand, depending on the branch of the ulnar nerve that is compressed.
Median nerve compression or Carpal tunnel syndrome:
Due to the compression of the median nerve occurs tingling in the thumb, index, middle and ring finger – is called carpal tunnel syndrome. The carpel tunnel is situated at the wrist which is surrounded by the carpal bones on the dorsum aspect and connective tissue on the ventral(front) side.
Carpal tunnel syndrome (CTS), occurs when the median nerve is compressed on the palm side of the wrist and also occurs the overuse injury of the hand. The area may become inflamed and narrow the tunnel that compresses the structures of carpal tunnel and due to that pain, tingling, or weakness in the thumb, fingers, and hand. The sensory and motor functions are affected in this condition. The flexor muscles are passes through the tunnel to the hand and that is responsible for the restriction of hand movement. The sensations are also altered in the thumb, index finger, middle finger, and half of the ring finger.
It is difficult to report the exact incidence rate for these both (median nerve compression and ulnar nerve palsy) non- traumatic conditions. These conditions are not more serious but if patients get ignored in an early stage or do not take proper treatment of it so the conditions become worsen. When a person feels some changes or difficulty in daily activity so they go to the doctor in an early period and get recover faster. The prevalence of hand and wrist non-traumatic conditions of both nerve (ulnar or median nerve) compression ranges from 10% to 70% mentioned in the literature.
Other factors which can affect the occurrence of cyclist’s palsy are:
Generally hand fatigue, because of increased weight bearing on the hands.
Don’t change the hand position on the handlebar frequently time.
Wear ill-fitted gloved hands.
Improper bike fit or position.
Improper shape or size of the handlebar which is not suitable for the cyclist.
More high or downward tilted saddle causes the improper distribution of body weight on the hands during holding the handlebar.
Diagnosis of cyclist palsy:
Diagnosis of Cyclist’s Palsy is based on the patient whole symptoms and taking a physical examination depending on it. When we know the exact place on the hand where the patient has a feeling of numbness, so we can differentiate between carpal tunnel syndrome and ulnar tunnel syndrome.
Physically differentiate the condition check by the special test of the particular nerve. Like Tinnels test, Forments test, Phalens test, Wartenberg sign, etc.
When suspected nerve damage, additional radiological tests such as ultrasound, CT-scan, and MRI can be performed to help confirm the diagnosis and determine the location and at which nerve is compressed.
Electrodiagnostics tests are the following:
X-rays: It is performed to evaluate any bone abnormality in the wrist along the whole nerve path.
NCV: A nerve conduction study (NCS) measures the severity of injury to the nerve.
MRI: It is used to evaluate another source of compression of the nerve at the wrist like a cyst or any fatty growth.
Electromyography (EMG): In this test measure the electrical activity of muscles (which is supplied by the particular nerve) during rest and the contraction period.
Differential diagnosis of cyclist palsy:
The nerve compression results from pressure generated during cycling, and many other injuries that can cause neuropathy in the wrist by nerve compression.
Other injuries are the following:
- Fracture of any wrist bone.
- Hypermobile pisiform bone.
- Occupational traumatic neuritis.
- Synovitis of the flexor tendons.
- Any type of uses wrist crutch.
- Osteoarthritis of the wrist or hand.
- As always in the assessment ask about to patient any recent trauma and any red flags.
These all are also responsible for the ulnar or median nerve compression in the wrist and symptoms are also the same so that by the special test, other investigations, and patient’s history doctor gives the confirmed diagnosis and differentiates the condition from any others.
Assessment for cyclist person:
Questions ask to the patient include:
Subjective Assessment:
Any type of hand problems in past?
Are any accidents falling off bikes in the past or present?
Check for any other factors of the body i.e recent malignancy, unremitting pain, weight loss, etc.
Is it a long-term or recent condition?
Person’s Bike Fit been done or not?
Recent changes in bike handlebars?
What type of work do they do?
Objective Assessment:
Bike position and person’s posture:
Assess the person on the bike:
- Cycling position
- Wrist position
- Forward leaning or too high seating
- Elbow joints locked out
- The Upper back is hunched
- Gripping strength
Upper limb assessment:
- Check the wrist and finger joint movements.
- Core muscle strength which responsible for stabilizing/supporting the upper limb.
- Forearm muscle strength.
- Wrist and hand muscles strength.
- Perform the Neurodynamic tests like ULTTs to define the particular nerve involvement.
Outcome Measures:
- Brigham and Women’s Carpal Tunnel Questionnaire
- VAS (Visual analog scale) for pain.
- Upper Extremity Functional Index
- DASH(Disability of arm, shoulder, and hand) outcome measure
Treatment for the cyclist palsy:
Cyclist’s palsy is a self-limiting condition and treatment is depending on the patient’s severity. first-line treatment of the medical treatment with physiotherapy treatment and if the severity is more so that another step is surgery.
Medical treatment:
- First, advise the take a rest and apply the ice to the pain area.
- Give the NSAIDs (Nonsteroidal inflammatory drugs) medication to treat the inflammation or reduce the pain.
- Wearing the splint decreases carpal tunnel syndrome’s symptoms.
- Soft tissue manipulation.
- Physiotherapy treatment
- Occupational therapy.
If the medical treatment is not useful or treatment fails so the doctor decides on the surgery.
Surgical treatment for Cyclist palsy:
The doctor gives a corticosteroid injection for the Guyon’s Canal or carpal tunnel condition or decompression surgery (the release of the pressure on the nerve).
Recovery from surgery can take up to six weeks, after removing the bandages within 24 hours, and stitches are removed in a week.
Ergonomic advice for cyclist palsy:
- Advice to the patient to body position and cycle or bike selection or it’s a position which they used.
- Cycle’s handlebars are proper in size according to the suitable for him.
- The seat height is proper.
- Back straight during cycling.
- The hand or wrist position is proper not too much in the extended position.
- Neck posture.
- Use properly padded handlebars of the cycle.
- Wearing padded gloves.
Physiotherapy Treatment for the cyclist palsy:
- Ice (cryotherapy)/ heat therapy.
- Electrical Stimulation for the affected nerve.
- Low-level laser therapy.
- Ultrasound
- Active release techniques, soft tissue massage.
- Active exercises of the Neck and Wrist.
- strengthening exercise of wist.
- stretching of wrist muscles.
Exercises for the Cyclist palsy:
Active exercise of the neck:
- Neck flexion movement: Patient neck is first in a neutral or straight position then ask the patient to see downward and then return to in a neutral position. And repeat 10 times.
- Neck extension movement: Ask the patient to see an upward or ceiling from the neutral neck position and repeat it for 10 times.
- Neck rotation movement: Ask the patient to rotate the whole neck in clockwise and anti-clockwise and repeat the 10 times.
- Neck sideward movement: First neck in a neutral position and ask the patient to do leaning or down the neck on the right side and then do the same on the left side. Repeat both side movements 10-10 times.
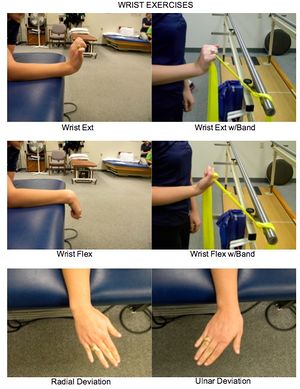
Active exercise of the wrist: This exercise does on a flat surface or on a table.
- Wrist flexion movement: Ask the patient to bend the wrist forward and then return to a neutral position. Hold the position for 5 seconds and repeat it 10 times.
- Wrist extension movement: Ask the patient to bend the wrist backward hold it for 5 sec and back to the neutral position. Repeat this exercise 10 times.
- Wrist deviation movement: Ask the patient to deviate the wrist to right and left on both sides and repeat it 10 times.
Hand Strengthening exercise:
- Finger bending exercise: It Starts from a stretched hand, bends or flexes your fingers of the affected hand at a right angle, and holds it for 10 seconds then keep your fingers straight, and repeats 5 times.
- Finger squeeze: The therapist give a small object (for example pen, coin, a sheet of paper) and places it between 2 fingers of the affected hand and holds for 10 seconds, repeat 5 times for each pair of fingers, and then go to the next fingers.
- Grip strengthening exercise: Take a rubber ball in the affected hand and squeeze it; hold for 10 seconds and repeat 10 times. Gradually do it to 3 sets of 10 repetitions.
Strengthening exercises will help to reoccur the cyclist’s condition.
Wrist flexor stretch:
- Extend your arm in front of you, then face your palm away from your body.
- Keep your hand towards the ceiling and bend your wrist backward.
- Use your other hand to gently bend your wrist backward until you feel a mild stretch in your forearm. Once the mild stretch relieves, add more pressure.
- Hold the wrist for 15-30 seconds
- Repeat up to 3 times.
Wrist extensors stretch:
- Extend your arm in front of you, then face your palm away from your body.
- Keep your hand downward and bend your wrist in front.
- Use your other hand to gently bend your wrist downwardly until you feel a mild stretch in your forearm. first the mild stretch relief, then add more pressure.
- Hold the wrist for 15-30 seconds
- Repeat up to 3 times.
How to Prevent the cyclist palsy?
- Lower seating position and adjust your seat backward to reduce stress to the arms and hands.
- Change your hand position frequently. And taking rest during the long route cycling.
- Wear hand gloves with padding. Keep the weight off the arms as possible,
- If you frequently ride on normal stationary bikes, use hoods to keep relaxed and decrease the risk of overuse injury.
- The therapist advised the patient that used a simple and postural adjustment bike to prevent the occurrence or reoccurrence of cyclist palsy.
One of the above whole techniques is able to prevent or resolve these hand and wrist symptoms.