TRIGGER POINT MASSAGE : FOR MUSCLES RELAXATION
Table of Contents
What is Trigger Point Massage?
- Trigger point therapy is a bodywork technique that involves the application of pressure to tender muscle tissue in order to relieve pain and dysfunction in other parts of the body. It may also be called myofascial (myo meaning muscle, fascial meaning connective tissue) trigger point therapy. Trigger point therapy is sometimes regarded as one of a group of treatment aproaches called neuromuscular therapy or NMT. Myotherapy , developed by Bonnie Prudden , is a related type of trigger point therapy.
- A Trigger Point (TrP) is a hyperirritable spot, a palpable nodule in the taut bands of the skeletal muscles’fascia.
Direct compression or muscle contraction can elicit jump sign, local tenderness, local twitch response and referred pain which usually responds with a pain pattern distant from the spot.
DESCRIPTION:
- Jump sign is the characteristic behavioral response to pressure on a TrP. Individuals are frequently startled by
the intense pain. They wince or cry out with a response seemingly out of proportion to the amount of pressure exerted by the examining fingers. They move involuntarily, jerking the shoulder, head, or some other part of the body not being palpated. A jump sign thus reflects the extreme tenderness of a TrP. This sign has been considered pathognomonic for the presence of TrPs. - Local twitch response – defined as a transient visible or palpable contraction of the muscle and skin as the tense muscle fibers contract when pressure is applied. Coursed by needle penetration or by transverse snapping palpation.
- Referred pain, also called reflective pain, is pain perceived at a location other than the site of the painful stimulus. Pain is reproducible and does not follow dermatomes, myotomes, or nerve roots. There is no specific joint swelling or neurological deficits. Pain from a myofascial TrP is a distinct, discrete and constant pattern or map of pain with no gender or racial differences able to reproduce symptoms.
- Typically, a health care professional refers a patient to a trigger point therapist. The therapist will take a history of injuries suffered, occupations held, and sports played. He or she will ask the individual to describe the pain and its location in detail.
- The therapist will then probe the area of the coordinating trigger point. An injection of lidocaine, saline, or other medicines, or probing with a dry needle, may be done. In myotherapy, once the point is found, the therapist will apply sustained pressure using the fingers, knuckles, or elbows for several seconds.
- Pain relief is often experienced immediately. Following the injection or pressure treatment, the therapist will then gently stretch the muscles of the trigger point. Finally, a series of exercises is taught to the individual to reeducate the muscles and to prevent the pain from returning.
ETIOLOGY:

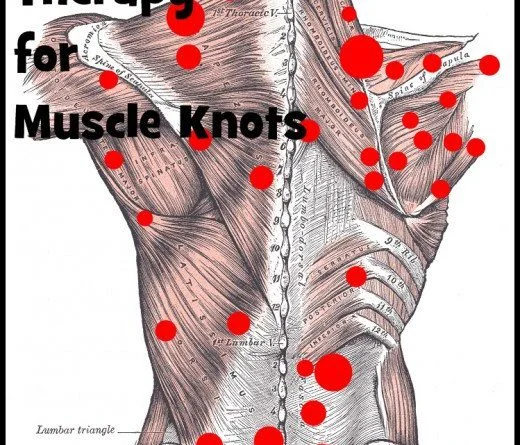
- Trigger points develop in the myofascia, mainly in the center of a muscle belly where the motor endplate enters
(primary or central TrPs).Those are palpable nodules within the tight muscle at the size of 2-10 mm and can demonstrate at different places in any skeletal muscles of the body. We all have TrPs in the body. Can be present even in babies and children, but their presence does not necessarily result in the formation of pain syndrome. When it happens,Trigger Points are directly associated with myofascial pain syndrome, somatic dysfunction, psychological disturbance and restricted daily functioning. - Myofascial Pain Syndrome refers to regional pain of soft tissue origin and is associated with muscle tenderness that arises from Trigger Points, focal points of tenderness, a few millimeters in diameter, found at multiple sites in a muscle and the fascia of muscle tissue.
Causes of Trigger Point:
– Aging,
– Injury sustained by a fall, by stress or birth trauma.
– Lack of exercise – commonly in sedentary persons between 27,5-55 years, of which 45% are men,
– Bad posture – upper and lower crossed pattern, swayback posture, telephone posture, cross-legged sitting,
– Muscle overuse and respective micro trauma – weightlifting,
– Chronic stress condition – anxiety, depression, psychological stress trauma,
– Vitamin deficiencies – vitamin C, D, B; folic acid; iron;
– Sleep disturbance,
– Joint problems and hyper-mobility.
Classification of Trigger Point:
1.Primary / Central AND Secondary / Satellite Trigger Points:
- Primary or Central Trigger Points are those that cause severe pain locally at the pressure with irradiation according
to referred pain map. Usually are based around the center of a muscle belly. - Secondary or Satellite Trigger Points arise in response to existing central trigger points in surrounding muscles.
- They usually spontaneously withdraw when the central Trigger Points is healed. Can be present in the form of a cluster.
2.Active AND Inactive /Latent Trigger Points:
- Active TrP is any point that causes tenderness and referral pain pattern on palpation. Almost always central
TrPs are active and some satellite TrPs are also active (but not necessarily all of them). Inactive TrPs can
eventually become active if there is a provocative factor. - Inactive or Latent TrPs can develop in anywhere and under fingertips feel like lumps, but are not painful.
Can increase a stiffness of the muscles.
3.Diffuse Trigger Points:
- Commonly happen in case of severe postural deformity where initially primary TrPs are multiple, so secondary
multiple TrPs are only a response of a mechanism, called diffuse.
4.Attachment Trigger Points:
- Arise in tendo-osseous junctions which become very tender. If not treated, degenerative processes of an
adjacent joint can spring up.
5.Ligamentous Trigger Points:
- Even ligaments can develop trigger points. Presence of TrPs in the anterior longitudinal ligament of the
spine can result in neck instability. Some knee pain syndromes are successfully healed when treated ligamentum patellae and fibular collateral ligament.

Symptoms of Trigger Point:
- A patient usually asks for help due to a chronic pain state (ex: headaches, aches everywhere, morning stiffness, TMJ syndrome, tinnitus), which, in reality, is often physically away from the active trigger point.
- Muscle weakness or imbalance, altered motor recruitment, in either the affected muscle or in functionally related muscles.
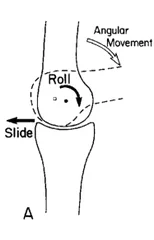
- Changes in Range of Motion (ROM).
- Painful movement and/or movement that sometimes can exacerbate symptoms.
- Tension headaches, migraines, tinnitus, temporomandibular joint problems… as accompanying symptoms.
Postural abnormalities and compensations.
Precaution:
- Persons with infectious diseases, open sores, or recent injuries should wait until they have recovered before beginning trigger point therapy.
- Persons taking anticoagulant prescription drugs may experience bruising after trigger point therapy.
Massage For Trigger Point:

- If possible, everyday-life factors that arouse the emergence of a TrPs must be eliminated or reduced,
- Posture training and education about postures and lifestyle,
- Passive stretching and/or Foam Roller stretching, few times a day,
- Self-massage, few times a day, and especially Deep Stroking Massage, done rhythmically and in only one direction,
- Strengthening: initially only isometric and then isotonic exercises,
- Ischemic Compression Technique – the term has been used to describe treatment in which ischemia is induced in the TrPt zone by applying sustained pressure. However, this principle is questionable, since the nucleus of the TrP intrinsically presents important hypoxia. Simons described a similar treatment modality, though without the need to induce additional ischemia in the TrP zone (TrP Pressure Release). The aim of this technique is to free the contracted sarcomeres within the TrP. The amount of pressure applied should suffice to produce gradual relaxation of the tension within the TrP zone, without causing pain. Yet both techniques show imitate significant improvement of the ROM after treatment.
- Taping Technique
- Spray and Stretch Technique by using ethyl chloride spray,
- Manual Lymphatic Drainage (MLD), since the presence of TrPs obstacle lymphatic flow,
- Other proprioceptive neuromuscular techniques: Reciprocal Inhibition (RI), Post-Isometric Relaxation (PIR), Contract-Relax/Hold-Relax (CRHR), Contract
- Relax/Antagonist Contract (CRAC),
- Some specific techniques like Neuromuscular Technique(NMT), Muscle Energy Technique (MET) and Myotherapy (MT),
- Ultrasonography, Hot and Cold packs, Short wave Diathermy– Tecar therapy, Laser, Ionophoresis.